

This methodological note describes the development and application of a mixed-methods protocol to assess the responsiveness of Spanish health systems to violence against women in Spain, based on the World Health Organization (WHO) recommendations.
Five areas for exploration were identified based on the WHO recommendations: policy environment, protocols, training, accountability/monitoring, and prevention/promotion. Two data collection instruments were developed to assess the situation of 17 Spanish regional health systems (RHS) with respect to these areas: 1) a set of indicators to guide a systematic review of secondary sources, and 2) an interview guide to be used with 26 key informants at the regional and national levels.
We found differences between RHSs in the five areas assessed. The progress of RHSs on the WHO recommendations was notable at the level of policies, moderate in terms of health service delivery, and very limited in terms of preventive actions. Using a mixed-methods approach was useful for triangulation and complementarity during instrument design, data collection and interpretation.
Esta nota metodológica describe el desarrollo de un protocolo de investigación que utiliza métodos mixtos para evaluar la respuesta del sistema sanitario español a la violencia contra las mujeres, partiendo de las recomendaciones de la Organización Mundial de la Salud (OMS).
A partir de estas recomendaciones, se definieron cinco áreas para su evaluación: políticas, protocolos, formación, rendición de cuentas/monitoreo, y acciones de prevención y promoción. Se desarrollaron dos instrumentos — un conjunto de indicadores para orientar la revisión sistemática de fuentes secundarias, y una guía de entrevista, que se utilizó con 26 informantes clave — y se aplicaron en los 17 sistemas sanitarios autonómicos.
Se evidenciaron diferencias entre autonomías y entre las cinco áreas evaluadas: notable progreso en políticas, menos destacado en la prestación de servicios y muy limitados en acciones preventivo-promocionales. Combinar métodos permitió lograr triangulación, complementariedad y desarrollo, durante el diseño de los instrumentos, la recogida de información y su interpretación.
The health sector plays an important role as part of an integrated response to violence against women (VAW).1 Women access health services more often than other public services, and proper training of health providers on VAW improves referral to specialist VAW services2 — where intensive advocacy interventions can be provided.3
Despite widespread recognition of the importance of the health sector in addressing VAW, there is little published research on how and to what extent regional or national health systems manage this issue.4 Despite the fact that methods exist to assess the responsiveness of providers and health facilities to VAW, there are few methodologies that assess responsiveness of entire health systems.4
This methodological note describes the development and application of a mixed methods approach to assess the responsiveness of Spanish health systems to VAW, based on the World Health Organization (WHO) recommendations.5
Applying the WHO recommendations to develop a research protocolThe WHO recommendations emerged from a 2009 expert meeting to develop guidelines for the health sector response to VAW. Experts from 20 countries attended, as did the Reproductive Health and Injury Prevention departments of WHO. Thirteen key elements were identified: 1) enabling environments, 2) training, 3) systems and services, 4) accountability and monitoring, 5) research and surveillance, 6) approaches to psychosocial support, 7) non-negotiable principles, 8) screening, 9) network development, 10) linking VAW with child protection, 11) mandatory reporting (straightforward regarding the importance of ensuring confidentiality and safety, and ambiguous regarding reporting without women's consent, 12) responding to men as victims and perpetrators, and 13) prevention and promotion.5
For this study, the 13 themes were adapted into five key areas: 1) enabling policy environment and networks, 2) protocols and guidelines for the healthcare response, 3) training of health professionals, 4) accountability and monitoring mechanisms, and 5) prevention and promotion.
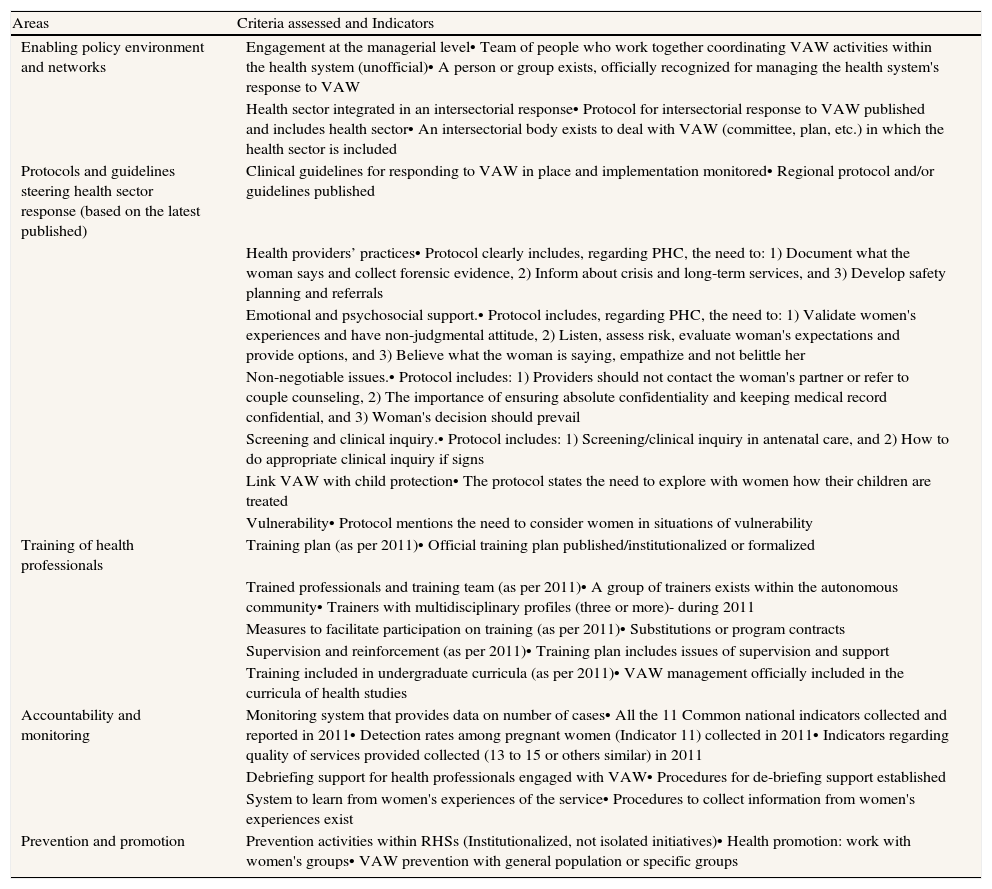
The five areas and selected indicators are shown in Table 1.
Set of indicators to evaluate regional health systems’ responsiveness - responses recorded as present or absent.
| Areas | Criteria assessed and Indicators |
| Enabling policy environment and networks | Engagement at the managerial level• Team of people who work together coordinating VAW activities within the health system (unofficial)• A person or group exists, officially recognized for managing the health system's response to VAW |
| Health sector integrated in an intersectorial response• Protocol for intersectorial response to VAW published and includes health sector• An intersectorial body exists to deal with VAW (committee, plan, etc.) in which the health sector is included | |
| Protocols and guidelines steering health sector response (based on the latest published) | Clinical guidelines for responding to VAW in place and implementation monitored• Regional protocol and/or guidelines published |
| Health providers’ practices• Protocol clearly includes, regarding PHC, the need to: 1) Document what the woman says and collect forensic evidence, 2) Inform about crisis and long-term services, and 3) Develop safety planning and referrals | |
| Emotional and psychosocial support.• Protocol includes, regarding PHC, the need to: 1) Validate women's experiences and have non-judgmental attitude, 2) Listen, assess risk, evaluate woman's expectations and provide options, and 3) Believe what the woman is saying, empathize and not belittle her | |
| Non-negotiable issues.• Protocol includes: 1) Providers should not contact the woman's partner or refer to couple counseling, 2) The importance of ensuring absolute confidentiality and keeping medical record confidential, and 3) Woman's decision should prevail | |
| Screening and clinical inquiry.• Protocol includes: 1) Screening/clinical inquiry in antenatal care, and 2) How to do appropriate clinical inquiry if signs | |
| Link VAW with child protection• The protocol states the need to explore with women how their children are treated | |
| Vulnerability• Protocol mentions the need to consider women in situations of vulnerability | |
| Training of health professionals | Training plan (as per 2011)• Official training plan published/institutionalized or formalized |
| Trained professionals and training team (as per 2011)• A group of trainers exists within the autonomous community• Trainers with multidisciplinary profiles (three or more)- during 2011 | |
| Measures to facilitate participation on training (as per 2011)• Substitutions or program contracts | |
| Supervision and reinforcement (as per 2011)• Training plan includes issues of supervision and support | |
| Training included in undergraduate curricula (as per 2011)• VAW management officially included in the curricula of health studies | |
| Accountability and monitoring | Monitoring system that provides data on number of cases• All the 11 Common national indicators collected and reported in 2011• Detection rates among pregnant women (Indicator 11) collected in 2011• Indicators regarding quality of services provided collected (13 to 15 or others similar) in 2011 |
| Debriefing support for health professionals engaged with VAW• Procedures for de-briefing support established | |
| System to learn from women's experiences of the service• Procedures to collect information from women's experiences exist | |
| Prevention and promotion | Prevention activities within RHSs (Institutionalized, not isolated initiatives)• Health promotion: work with women's groups• VAW prevention with general population or specific groups |
For each of these areas, two data collection instruments were developed: 1) a set of indicators, to guide the systematic review of secondary sources, and 2) an interview guide, to be used during semi-structured interviews with key informants (Appendix A).
The settingSpain's Gender Violence Law of 2004 strengthened the role of health services regarding VAW: possible cases should be identified, managed, and addressed through a multidisciplinary response.6 The National Commission Against Gender-Based Violence (NCAGBV) was created within the Inter-territorial Council of the National Health System. Three actions are indicated to facilitate integration of VAW nationally and within the autonomous regional health systems (RHSs): 1) development of protocols, 2) training of health professionals, and 3) development of information systems- based on 11 national common indicators for monitoring VAW cases detected within health facilities. At the regional level, delegates to the NCAGBV and civil servants are responsible for the coordination of these actions.
We included 17 Spanish RHSs in this study; the autonomous regions of Ceuta and Melilla were excluded.
Using mixed-methods to refine the protocol instruments and collect informationAccording to Johnson et al. a mixed methods research approach is useful for triangulation, complementarity, development, initiation and expansion.7
Data collected through individual interviews served to triangulate and complement the information gathered through the documentary review. Mixed methods were useful for developing the data collection instruments. Information from the interviews facilitated further development of the indicators to be assessed, while data collected through documentary review served to further develop the interview guides.
Content analysis of secondary sourcesSecondary sources were systematically reviewed through content analysis to assess each indicator for each of the 17 RHSs. Regional documents reviewed included VAW laws and health plans and protocols, and national documents included the Ministry of Health Gender Violence Reports for the years 2005-2011. Documents were retrieved through the internet, focusing mainly on official health-related websites of the autonomous regions and the NCAGBV. Hard copies of certain documents (i.e. training programs) were collected and revised. For each RHS, indicators were assessed as present or absent.
Interviews with key informantsIndividual interviews were conducted with 26 key informants: 23 from the 17 RHSs and 3 at the national level. Informants in the autonomous regions were civil servants of the RHSs in charge of coordinating the health-sector response to VAW. One key-informant per autonomous region was contacted first. In some regions another informant was suggested due to his/her experience in certain areas of interest to the study. Informants at the national level were representatives of the Observatory of Women's Health and academic institutions. They were all participants in working groups on VAW and some of them had also participated in the NCAGBV. They were chosen based on their status as privileged informants — able to contribute significantly to our research- through theoretical sampling. Fifteen of the interviews were conducted face to face, 11 were phone interviews, and the average duration was one hour.
Interviews were semi-structured and followed a guide. As unexpected issues emerged they were explored in subsequent interviews following an emergent design.8 Verbatim transcripts were analyzed using qualitative content analysis, focusing on the manifest content.9
The study was approved by the Ethical Committee of the University of Alicante. Written informed consent was obtained from each participant before interviews were conducted. Information that could identify the respondents was excluded.
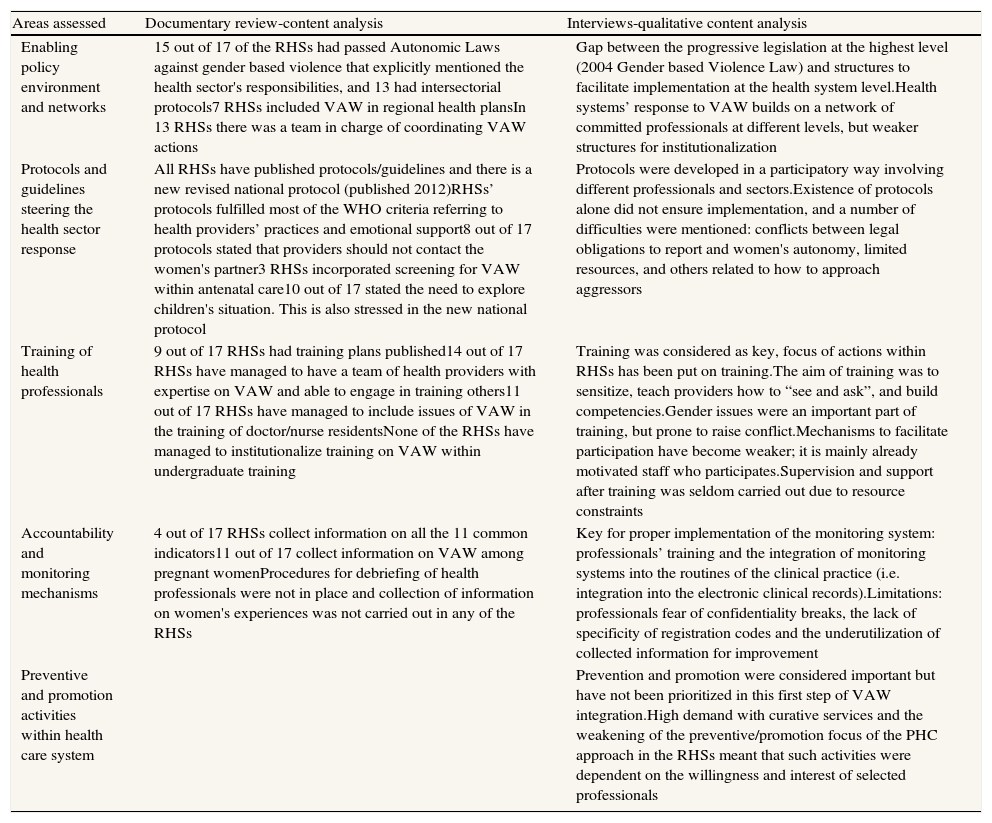
Preliminary findings from the application of the methodologyThe methodology mapped differences between RHSs, in terms of documentation and levels of achievement in the five assessed areas. Progress was notable at the level of policies and protocols, moderate at the level of health service delivery, and very limited in terms of the institutionalization of action on prevention and promotion. A summary of findings is presented in Table 2.
Preliminary findings from the application of the methodology to assess Spain's Regional Health System's response to violence against women.
| Areas assessed | Documentary review-content analysis | Interviews-qualitative content analysis |
| Enabling policy environment and networks | 15 out of 17 of the RHSs had passed Autonomic Laws against gender based violence that explicitly mentioned the health sector's responsibilities, and 13 had intersectorial protocols7 RHSs included VAW in regional health plansIn 13 RHSs there was a team in charge of coordinating VAW actions | Gap between the progressive legislation at the highest level (2004 Gender based Violence Law) and structures to facilitate implementation at the health system level.Health systems’ response to VAW builds on a network of committed professionals at different levels, but weaker structures for institutionalization |
| Protocols and guidelines steering the health sector response | All RHSs have published protocols/guidelines and there is a new revised national protocol (published 2012)RHSs’ protocols fulfilled most of the WHO criteria referring to health providers’ practices and emotional support8 out of 17 protocols stated that providers should not contact the women's partner3 RHSs incorporated screening for VAW within antenatal care10 out of 17 stated the need to explore children's situation. This is also stressed in the new national protocol | Protocols were developed in a participatory way involving different professionals and sectors.Existence of protocols alone did not ensure implementation, and a number of difficulties were mentioned: conflicts between legal obligations to report and women's autonomy, limited resources, and others related to how to approach aggressors |
| Training of health professionals | 9 out of 17 RHSs had training plans published14 out of 17 RHSs have managed to have a team of health providers with expertise on VAW and able to engage in training others11 out of 17 RHSs have managed to include issues of VAW in the training of doctor/nurse residentsNone of the RHSs have managed to institutionalize training on VAW within undergraduate training | Training was considered as key, focus of actions within RHSs has been put on training.The aim of training was to sensitize, teach providers how to “see and ask”, and build competencies.Gender issues were an important part of training, but prone to raise conflict.Mechanisms to facilitate participation have become weaker; it is mainly already motivated staff who participates.Supervision and support after training was seldom carried out due to resource constraints |
| Accountability and monitoring mechanisms | 4 out of 17 RHSs collect information on all the 11 common indicators11 out of 17 collect information on VAW among pregnant womenProcedures for debriefing of health professionals were not in place and collection of information on women's experiences was not carried out in any of the RHSs | Key for proper implementation of the monitoring system: professionals’ training and the integration of monitoring systems into the routines of the clinical practice (i.e. integration into the electronic clinical records).Limitations: professionals fear of confidentiality breaks, the lack of specificity of registration codes and the underutilization of collected information for improvement |
| Preventive and promotion activities within health care system | Prevention and promotion were considered important but have not been prioritized in this first step of VAW integration.High demand with curative services and the weakening of the preventive/promotion focus of the PHC approach in the RHSs meant that such activities were dependent on the willingness and interest of selected professionals |
This study is the first attempt to translate WHO recommendations on the health sector response to VAW into a protocol to assess health system responsiveness to VAW. It should be noted that the latest WHO guidelines (outlined in the document “Responding to intimate partner violence and sexual violence against women”10) were not available at the time of this study, therefore the WHO Expert Meeting on Health Sector Responses to VAW was used as a guide. Our subsequent review of the new guidelines shows general alignment with the fields assessed and indicators used in our study.
Using a mixed methods approach was useful for the development of instruments, data collection and interpretation of results. The documentary review offered interesting information on differences among RHSs, but left important issues un-informed, for example, processes and quality monitoring, and aspects of prevention and promotion. Information collected through the interviews allowed us to put information into context and understand differences between RHSs in each of the five areas. It should be noted that there could be differences in the information collected by phone as compared to face-to-face. However, both phone and face-to-face interviews covered the same aspects and had similar durations.
This methodology was applied to the Spanish context, but it could be used to assess health system responsiveness in other settings as it permits detecting differences between health systems and conducting in-depth analysis, and because it is grounded in international standards.
Editor in charge of the articleGlòria Pérez.
Contributions of authorshipIsabel Goicolea conceived and designed the study, participated in data collection, analysis and interpretation, wrote the first draft of the paper and subsequent revisions and approved the final version.
Carmen Vives Cases and Ann Öhman participated in the design of the study, and the interpretation of the data, critically reviewed drafts of the paper and approved its final version.
Fauhn Minvielle and Erica Briones-Vozmediano participated in data collections, analysis and interpretation, critically reviewed drafts of the paper and approved its final version.
FundingThis study has been funded by a COFAS grant (supported by COFUND action within the Marie Curie Action People, in the Seventh Framework programme and the Swedish Council for Working Life and Social Research/FAS-Forskningsradet för arbetsliv och socialvetenskap).
Conflicts of interestThe second author belongs to the current editorial committee of Gaceta Sanitaria.
The authors are grateful to the Observatory of Women's Health of the Spanish Ministry of Health for facilitating access to relevant information and contacts, and to the Public Health Research Group of the Department of Community Nursing, Preventive Medicine and Public Health and History of Science of the Alicante of University (Spain), especially to Gaby Ortiz and Jordi Torrubiano for their support and feedback during the development of the study protocol. The authors are particularly grateful to Asunción Cisneros, Mari Luz Lou, Borja Rodriguez-Maribona, Alejandra Carmona, Rosa del Valle, Carmen Fernandez, Maria José López, Marisa Pires, Marina Tourné, and all the participants in the 17 autonomous regions and at the national level who shared their time, enthusiasm, experiences and expertise, and facilitated access to unpublished documents and information.









