


To develop a Spanish version of the WHO-Composite International Diagnostic Interview (WHO-CIDI) applicable to Spain, through cultural adaptation of its most recent Latin American (LA v 20.0) version.
MethodsA 1-week training course on the WHO-CIDI was provided by certified trainers. An expert panel reviewed the LA version, identified words or expressions that needed to be adapted to the cultural or linguistic norms for Spain, and proposed alternative expressions that were agreed on through consensus. The entire process was supervised and approved by a member of the WHO-CIDI Editorial Committee. The changes were incorporated into a Computer Assisted Personal Interview (CAPI) format and the feasibility and administration time were pilot tested in a convenience sample of 32 volunteers.
ResultsA total of 372 questions were slightly modified (almost 7% of approximately 5000 questions in the survey) and incorporated into the CAPI version of the WHO-CIDI. Most of the changes were minor — but important — linguistic adaptations, and others were related to specific Spanish institutions and currency. In the pilot study, the instrument's mean completion administration time was 2h and 10min, with an interquartile range from 1.5 to nearly 3h. All the changes made were tested and officially approved.
ConclusionsThe Latin American version of the WHO-CIDI was successfully adapted and pilot-tested in its computerized format and is now ready for use in Spain.
Desarrollar la versión española de la WHO-Composite International Diagnostic Interview (WHO-CIDI) para su uso en España mediante la adaptación cultural de la versión latinoamericana más reciente disponible (LA; v 20.0).
MétodosSe realizó un curso de una semana impartido por entrenadores certificados. Un panel de expertos revisó la versión latinoamericana e identificó las palabras o expresiones que requerían ser adaptadas a las normas culturales o linguísticas de España y se propusieron, por consenso, palabras o expresiones alternativas. El proceso fue supervisado y aprobado por un miembro del Comité Editorial de la WHO-CIDI. Los cambios fueron implementados en el formato informatizado CAPI (Computer Assisted Personal Interview). Un estudio piloto en una muestra de conveniencia de 32 voluntarios permitió calcular los tiempos de administración y viabilidad.
Resultados372 preguntas fueron modificadas (alrededor de un 7% del total de 5000 preguntas del instrumento completo) e implementadas en la versión CAPI de la WHO-CIDI. La mayoría de las modificaciones fueron adaptaciones lingüísticas menores, pero importantes, y otras se relacionaron con los recursos específicos de España y adaptaciones a la moneda utilizada. En el estudio piloto, la mediana del tiempo de duración de la WHO-CIDI completa fue de 2 horas y 10 minutos, con un rango intercuartil entre 1 hora y 25 minutos y casi 3 horas. Todos los cambios implementados fueron comprobados y aprobados oficialmente.
ConclusionesLa version latinoamericana de la WHO-CIDI ha sido adaptada y el formato informático ha sido pilotado con éxito, estando disponible para su utilización en España.
In the last three decades, the field of psychiatric epidemiology has rapidly expanded. One of the contributing factors to this development has been the progressive design, development and application of various highly structured and standardized diagnostic interviews which can be used by lay interviewers with no formal clinical training.1,2 In the early 1980s, the Diagnostic Interview Schedule (DIS) was the first structured clinical diagnostic interview specifically designed for use by lay trained interviewers who were not clinicians and its purpose was to generate accurate clinical psychiatric diagnoses using computerized algorithms based on the American Psychiatric Association (APA) Diagnostic and Statistical Manual of Mental Disorders 3rd edition (DSM-III) criteria. This instrument was used in the Epidemiologic Catchment Area (ECA) study, the first United States (U.S.) national survey conducted from 1981 to 1984 that ascertained prevalence rates and risk factors of mental disorders in the U.S.3 This landmark project led to replications in other countries as well as to the development of other structured diagnostic interviews, most notably the World Health Organization Composite International Diagnostic Interview (WHO-CIDI, hereafter referred to as CIDI), currently the most widely used mental health diagnostic interview worldwide.4 The CIDI was designed by the World Health Organization (WHO) for the purpose of ascertaining diagnoses based on definitions and criteria based on the WHO International Classification of Disease (ICD) and not exclusively on DSM definitions and criteria. This was particularly important for cross-national comparative research of epidemiological studies of mental illnesses since the ICD is the most widely used international classification system.
The International Consortium of Psychiatric Epidemiology, ICPE (http://www.hcp.med.harvard.edu/icpe/),5 funded by the U.S. National Institute of Mental Health (NIMH) used the CIDI as the diagnostic tool to facilitate cross-national comparisons of epidemiological surveys of mental illness in the general population. The ICPE was the precursor to the WHO sponsored World Mental Health (WMH) Surveys, which initiated in 1999. The primary aim of the WMH Surveys Consortium is to obtain objective estimates of the prevalence of mental disorders, their associated disability, and patterns of treatment by: (1) assessing the global burden of mental disorders; (2) determining the psychosocial risk factors and correlates of mental disorders; (3) establishing mental health utilization patterns; and (4) identifying modifiable barriers to help-seeking by carring out surveys in a representative number of countries in all major regions of the world.6 This consortium has coordinated the performance of CIDI surveys in the general population in more than 28 countries in all continents (http://www.hcp.med.harvard.edu/wmh), including many in Latin America such as México,7,8 Colombia9 and Perú.10 In this context, the European Study of the Epidemiology of Mental Disorders (ESEMeD) surveys11,12 coordinated the participation of six European countries (Belgium, France, Germany, Italy, Holland and Spain), which was a result of the ICPE experience.
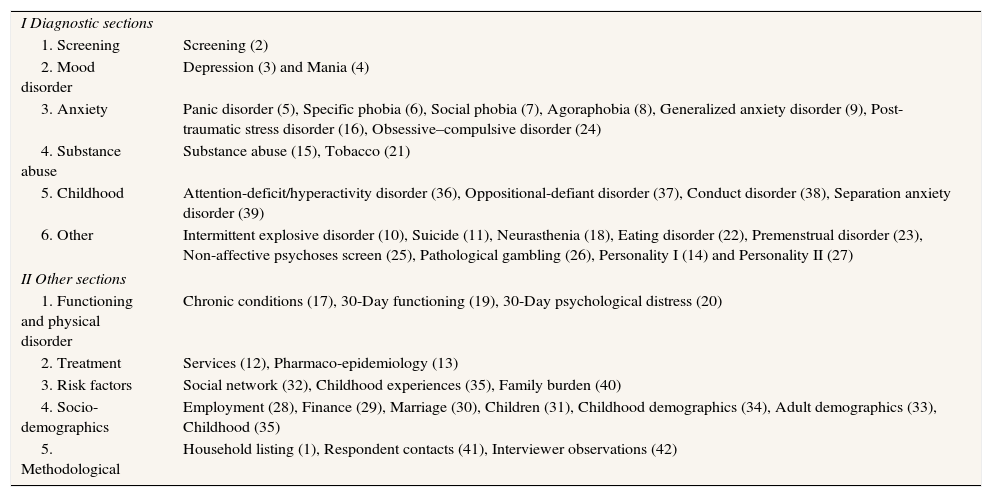
The WHO-Composite International Diagnostic Interview (WHO-CIDI)The CIDI is a comprehensive and highly-structured interview that comprises nearly 5000 questions divided into 42 sections,4,5,10 and these, in turn, are grouped into two main parts: diagnostic and other sections (Tables 1 and 2). The first includes the clinical part of the interview with an introductory screening section and 22 diagnostic sections that assess different psychiatric conditions. Unlike the rest of the clinical sections which provide ICD or DSM diagnoses, it is recommended that the psychosis section (section number 25)13 and the personality I and II (sections 14 and 27) are used only as screening instruments in the detection of psychosis and personality disorders in general population surveys. The second part includes various (non-clinical) sections which assess utilization of services, use of psychopharmacs, various kinds of functioning, physical chronic conditions, risk factors, social networks, caregiver burden and sociodemographic variables. Some of the sections are used to help establish methodological aspects, such as the selection of the interviewee from the previously chosen household. CIDI is available in two formats: the paper form or PAPI (Paper and Pencil Interviewing) and the computerized form or CAPI. The latter was designed to ease the handling of elaborate skip and complex randomization patterns and to facilitate data entry with a resulting reduction in interview time and errors in data collection and recording.
Schematic description of the World Health Organization-Composite International Diagnostic Interview (WHO-CIDI).a
| I Diagnostic sections | |
| 1. Screening | Screening (2) |
| 2. Mood disorder | Depression (3) and Mania (4) |
| 3. Anxiety | Panic disorder (5), Specific phobia (6), Social phobia (7), Agoraphobia (8), Generalized anxiety disorder (9), Post-traumatic stress disorder (16), Obsessive–compulsive disorder (24) |
| 4. Substance abuse | Substance abuse (15), Tobacco (21) |
| 5. Childhood | Attention-deficit/hyperactivity disorder (36), Oppositional-defiant disorder (37), Conduct disorder (38), Separation anxiety disorder (39) |
| 6. Other | Intermittent explosive disorder (10), Suicide (11), Neurasthenia (18), Eating disorder (22), Premenstrual disorder (23), Non-affective psychoses screen (25), Pathological gambling (26), Personality I (14) and Personality II (27) |
| II Other sections | |
| 1. Functioning and physical disorder | Chronic conditions (17), 30-Day functioning (19), 30-Day psychological distress (20) |
| 2. Treatment | Services (12), Pharmaco-epidemiology (13) |
| 3. Risk factors | Social network (32), Childhood experiences (35), Family burden (40) |
| 4. Socio-demographics | Employment (28), Finance (29), Marriage (30), Children (31), Childhood demographics (34), Adult demographics (33), Childhood (35) |
| 5. Methodological | Household listing (1), Respondent contacts (41), Interviewer observations (42) |
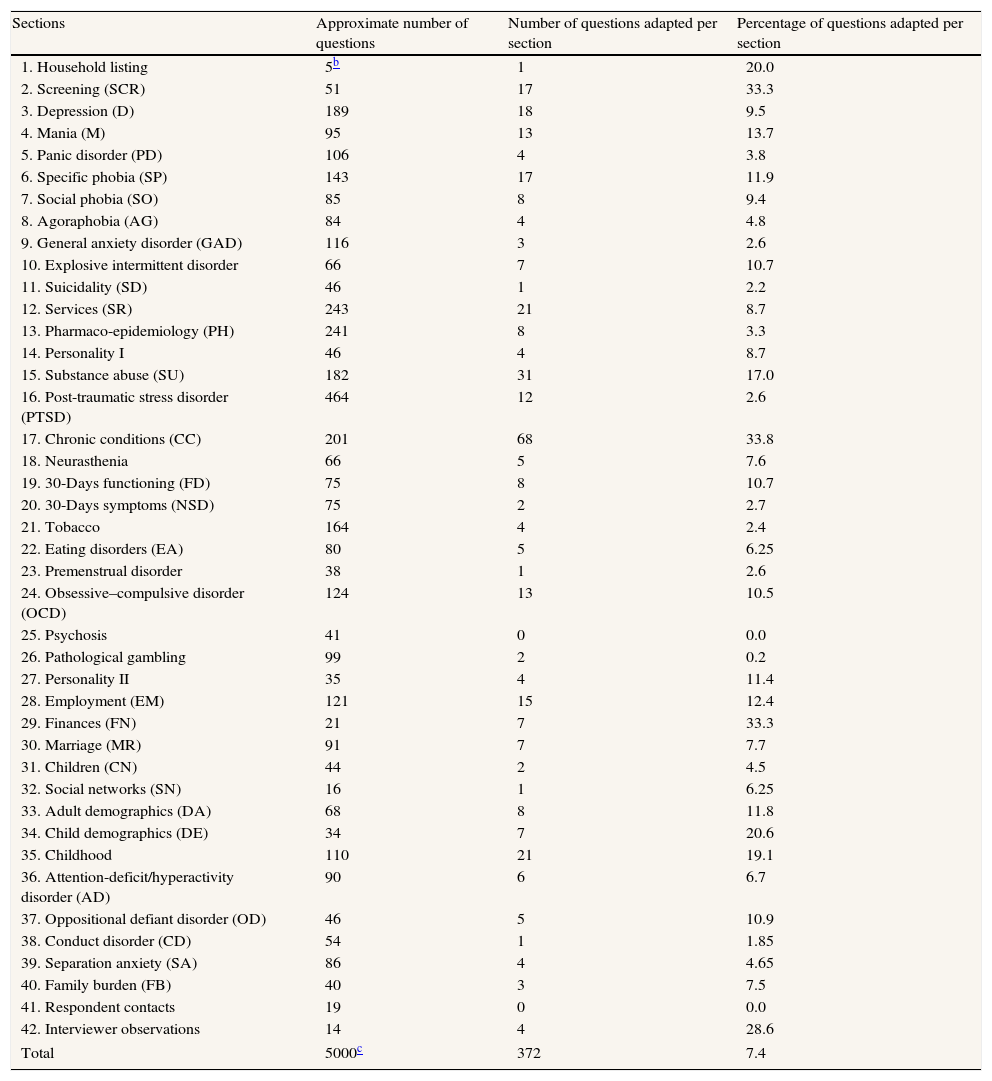
Description of the adaptations made in the different sectionsa of the WHO-Composite International Diagnostic Interview (WHO-CIDI).
| Sections | Approximate number of questions | Number of questions adapted per section | Percentage of questions adapted per section |
| 1. Household listing | 5b | 1 | 20.0 |
| 2. Screening (SCR) | 51 | 17 | 33.3 |
| 3. Depression (D) | 189 | 18 | 9.5 |
| 4. Mania (M) | 95 | 13 | 13.7 |
| 5. Panic disorder (PD) | 106 | 4 | 3.8 |
| 6. Specific phobia (SP) | 143 | 17 | 11.9 |
| 7. Social phobia (SO) | 85 | 8 | 9.4 |
| 8. Agoraphobia (AG) | 84 | 4 | 4.8 |
| 9. General anxiety disorder (GAD) | 116 | 3 | 2.6 |
| 10. Explosive intermittent disorder | 66 | 7 | 10.7 |
| 11. Suicidality (SD) | 46 | 1 | 2.2 |
| 12. Services (SR) | 243 | 21 | 8.7 |
| 13. Pharmaco-epidemiology (PH) | 241 | 8 | 3.3 |
| 14. Personality I | 46 | 4 | 8.7 |
| 15. Substance abuse (SU) | 182 | 31 | 17.0 |
| 16. Post-traumatic stress disorder (PTSD) | 464 | 12 | 2.6 |
| 17. Chronic conditions (CC) | 201 | 68 | 33.8 |
| 18. Neurasthenia | 66 | 5 | 7.6 |
| 19. 30-Days functioning (FD) | 75 | 8 | 10.7 |
| 20. 30-Days symptoms (NSD) | 75 | 2 | 2.7 |
| 21. Tobacco | 164 | 4 | 2.4 |
| 22. Eating disorders (EA) | 80 | 5 | 6.25 |
| 23. Premenstrual disorder | 38 | 1 | 2.6 |
| 24. Obsessive–compulsive disorder (OCD) | 124 | 13 | 10.5 |
| 25. Psychosis | 41 | 0 | 0.0 |
| 26. Pathological gambling | 99 | 2 | 0.2 |
| 27. Personality II | 35 | 4 | 11.4 |
| 28. Employment (EM) | 121 | 15 | 12.4 |
| 29. Finances (FN) | 21 | 7 | 33.3 |
| 30. Marriage (MR) | 91 | 7 | 7.7 |
| 31. Children (CN) | 44 | 2 | 4.5 |
| 32. Social networks (SN) | 16 | 1 | 6.25 |
| 33. Adult demographics (DA) | 68 | 8 | 11.8 |
| 34. Child demographics (DE) | 34 | 7 | 20.6 |
| 35. Childhood | 110 | 21 | 19.1 |
| 36. Attention-deficit/hyperactivity disorder (AD) | 90 | 6 | 6.7 |
| 37. Oppositional defiant disorder (OD) | 46 | 5 | 10.9 |
| 38. Conduct disorder (CD) | 54 | 1 | 1.85 |
| 39. Separation anxiety (SA) | 86 | 4 | 4.65 |
| 40. Family burden (FB) | 40 | 3 | 7.5 |
| 41. Respondent contacts | 19 | 0 | 0.0 |
| 42. Interviewer observations | 14 | 4 | 28.6 |
| Total | 5000c | 372 | 7.4 |
The most recent version of the CIDI (version 3.0) is the end result of a number of international studies and adaptations made since 2000 when the CIDI was first used in the WMH Surveys. It was first created in English and has been translated to more than 30 different languages using the standard WHO protocol with a rigorous process of adaptation in order to obtain conceptually and cross-culturally comparable versions in each of the target countries/languages that included forward and backward translations, review by expert panels, pre-testing using cognitive interview, debriefing techniques, and focus groups.11,14 Several clinical reappraisal studies have been carried out and the concordance of the CIDI version 3.0 has been evaluated in different probability samples of the WMH surveys (France, Italy, Spain and US) with the Structured Clinical Interview for DSM-IV (SCID) as the standardized clinical assessment. A moderate to excellent CIDI-SCID concordance has been found of most mental disorders.15,16 The original Spanish version used in Spain had not been updated since it was used in the context of the ESEMeD project ten years ago. All improvements to the instrument had been added to the Latin American (LA) version, so that the CIDI Latin American (LA) v 20.0 is the CIDI version 3.0 currently used in Spanish-speaking countries (e.g., Colombia). However, due to linguistic and cultural differences in Spanish-speaking target populations, there are some adaptations that needed to be made in applying the CIDI LA v 20.0 in Spain to take into account these differences and to ensure the semantic, idiomatic, experimental and conceptual equivalence.17,18
The aim of our work was the cultural adaptation of the LA CAPI version (v.20.0) of the CIDI instrument (version 3.0) for use in Spain. This was carried out as the first step of the PEGASUS-Murcia (Psychiatric Enquiry to General Population in Southeast Spain-Murcia) project, a general adult population survey of the prevalence of mental illness and its associated psychological, biological and social risk factors in the Murcia Region of Spain.
MethodsThe cultural and linguistic adaptation process of the CIDI follows a protocol-based pathway and has to be accepted and supervised by the editorial committee of WHO-CIDI.14 In brief, it comprises the following stages (Fig. 1): (1) formal training and accreditation for its use; (2) evaluation of the diagnostic interview by an expert panel; (3) formal acceptance of the proposed changes; (4) adaptation of the software for the CAPI format; and (5) pilot testing the instrument.

The training course for the researchers and interviewers was held in Murcia in December 2008 and was led by a trainer from the WHO-CIDI Training and Reference Centre (TRC) of Mexico and California (http://www.hcp.med.harvard.edu/wmhcidi/trc_americas.php). It comprised a five-day intensive course in which 15 interviewers and supervisors were trained in the use of the instrument. Four researchers were, simultaneously, accredited as trainers for future interviewers exclusively within the PEGASUS-Murcia project. Similarly, an information technology (IT) expert from the National Psychiatric Institute of Mexico trained a Bioestatistician and two IT experts in the use of the software, quality control algorithms and ascertaining diagnosis and statistics.
Stage 2: Evaluation of the questionnaireFull and meticulous review of the CIDI was carried out in three phases. First, one of the researchers carefully reviewed the instrument before the training course, identifying words or phrases which, in her opinion, did not fit with Spanish cultural and linguistic norms and customs. Second, the instrument was again reviewed during the CIDI training course by the four participating researchers. All of the interview sections were carefully examined during the intensive course, under the supervisión of the Latin-American WHO-CIDI expert, permitting a productive interaction between all of them. Finally, at the end of the course, another panel of experts from the research project carried out a further review of the document which had incorporated all the proposed changes. When disagreement about some of the suggested alternatives emerged, a consensus was reached and the final document was approved by the research team. During the entire process, the expert committee had complete access to both original English and Spanish versions (used in the ESEMeD project) of the CIDI (version 3.0).
Stage 3: Formal approval of the proposed changesThis final document was further examined by the Latin American and Caribbean coordinator of the WMH Survey Initiative and member of the CIDI editorial committee, and, following some minor revisions, it received full approval.
Stage 4: Adaptation of the software for the Computer Assisted Personal Interview (CAPI) versionThis revised final version was implemented in the CAPI format by the IT expert using the Blaise program, a flexible interviewing application used as a survey processing tool and developed by Statistics Netherlands (http://www.blaise.com/).
Stage 5: Pilot studyBetween May and June 2009, a sample of 32 volunteers was contacted to pilot test the diagnostic instrument. The researchers chose volunteers of different ages and emotional states to check any word or concept that should be clarified and to allow the testing of all the sections of the instrument. As not having a sufficient knowledge of Spanish speaking skills is considered as an exclusion criterion in this type of surveys, they were not included in the pilot study. The expected number of mental health cases in the pilot study was extremely low (N=2), considering a prevalence of any mental illness in the Spanish general population of 5.25%,19 so that the diagnostic algorithms were not run. The electronic information system recorded all information that was inputted to the computer with the corresponding times in a way that calculated the administration time of all and every section followed by the use of algorithms for the response consistency checks, originally developed using the statistics package SAS (Statistical Analysis System).
This study, as part of the PEGASUS-Murcia project, was approved by a local medical ethics advisory committee from Virgen de la Arrixaca Hospital.
ResultsAs part of the cultural and linguistic adaptation process of the Latin American version of the CIDI for its use in Spain, adaptations and changes were made to a total of 372 questions (approximately 7.4% of the total) with a mean of nine per section (standard deviation of 11.57), range from zero (Psychosis and Respondent Contacts sections) to 68 (34%) (Chronic Conditions section) (Table 2).
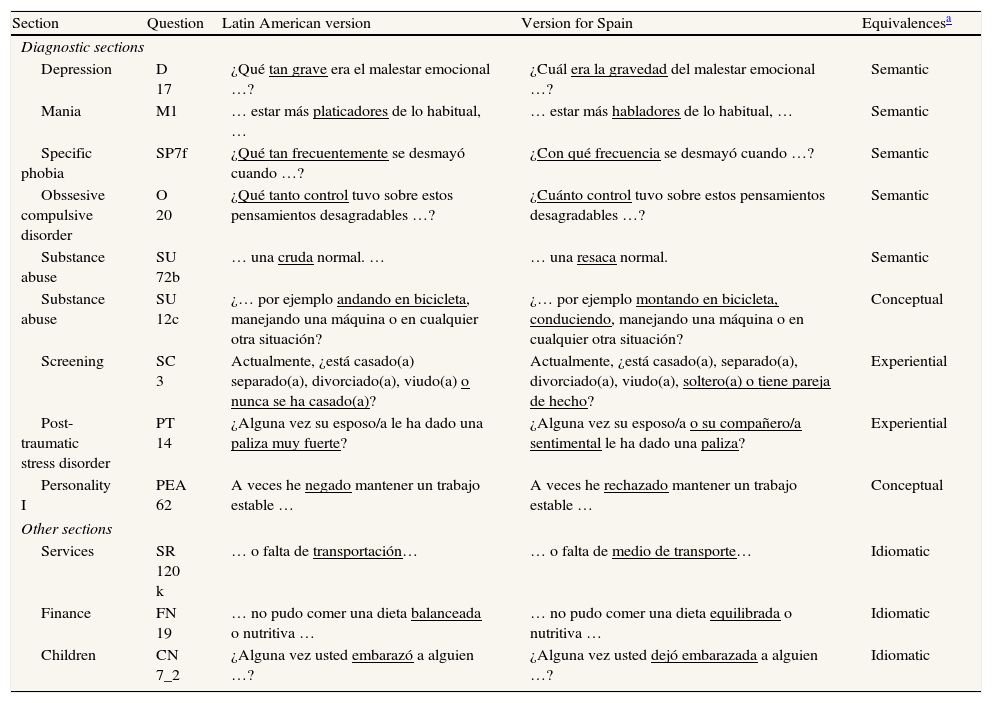
The majority of changes made were minor linguistic adaptations related to grammatical terms or vocabulary unique to Spain (semantic of idiomatic equivalences) (Table 3). Others needed a modification to capture experiential or conceptual equivalences more appropriate in Spain. For example, the expert panel considered that the psychological consequences of being beaten up by a spouse or romantic partner is not a matter of the intensity of the beat (badly beaten in PT14, Table 3), but they are related to the experience itself. Consistently, the adjective “muy fuerte” was eliminated looking for an experiential equivalence in Spain.
Examples of the minor cultural and linguistic adaptations included in the WHO-CIDI version for use in Spain.
| Section | Question | Latin American version | Version for Spain | Equivalencesa |
| Diagnostic sections | ||||
| Depression | D 17 | ¿Qué tan grave era el malestar emocional …? | ¿Cuál era la gravedad del malestar emocional …? | Semantic |
| Mania | M1 | … estar más platicadores de lo habitual, … | … estar más habladores de lo habitual, … | Semantic |
| Specific phobia | SP7f | ¿Qué tan frecuentemente se desmayó cuando …? | ¿Con qué frecuencia se desmayó cuando …? | Semantic |
| Obssesive compulsive disorder | O 20 | ¿Qué tanto control tuvo sobre estos pensamientos desagradables …? | ¿Cuánto control tuvo sobre estos pensamientos desagradables …? | Semantic |
| Substance abuse | SU 72b | … una cruda normal. … | … una resaca normal. | Semantic |
| Substance abuse | SU 12c | ¿… por ejemplo andando en bicicleta, manejando una máquina o en cualquier otra situación? | ¿… por ejemplo montando en bicicleta, conduciendo, manejando una máquina o en cualquier otra situación? | Conceptual |
| Screening | SC 3 | Actualmente, ¿está casado(a) separado(a), divorciado(a), viudo(a) o nunca se ha casado(a)? | Actualmente, ¿está casado(a), separado(a), divorciado(a), viudo(a), soltero(a) o tiene pareja de hecho? | Experiential |
| Post-traumatic stress disorder | PT 14 | ¿Alguna vez su esposo/a le ha dado una paliza muy fuerte? | ¿Alguna vez su esposo/a o su compañero/a sentimental le ha dado una paliza? | Experiential |
| Personality I | PEA 62 | A veces he negado mantener un trabajo estable … | A veces he rechazado mantener un trabajo estable … | Conceptual |
| Other sections | ||||
| Services | SR 120 k | … o falta de transportación… | … o falta de medio de transporte… | Idiomatic |
| Finance | FN 19 | … no pudo comer una dieta balanceada o nutritiva … | … no pudo comer una dieta equilibrada o nutritiva … | Idiomatic |
| Children | CN 7_2 | ¿Alguna vez usted embarazó a alguien …? | ¿Alguna vez usted dejó embarazada a alguien …? | Idiomatic |
The equivalences achieved by the expert committee were grouped in four areas: semantic equivalence (grammatical difficulties or looking for the same meaning); idiomatic equivalences (colloquialisms or idioms difficult to understand); experiential equivalence (trying to capture and experience of daily life in different cultures); and conceptual equivalences (different conceptual meanings between cultures).
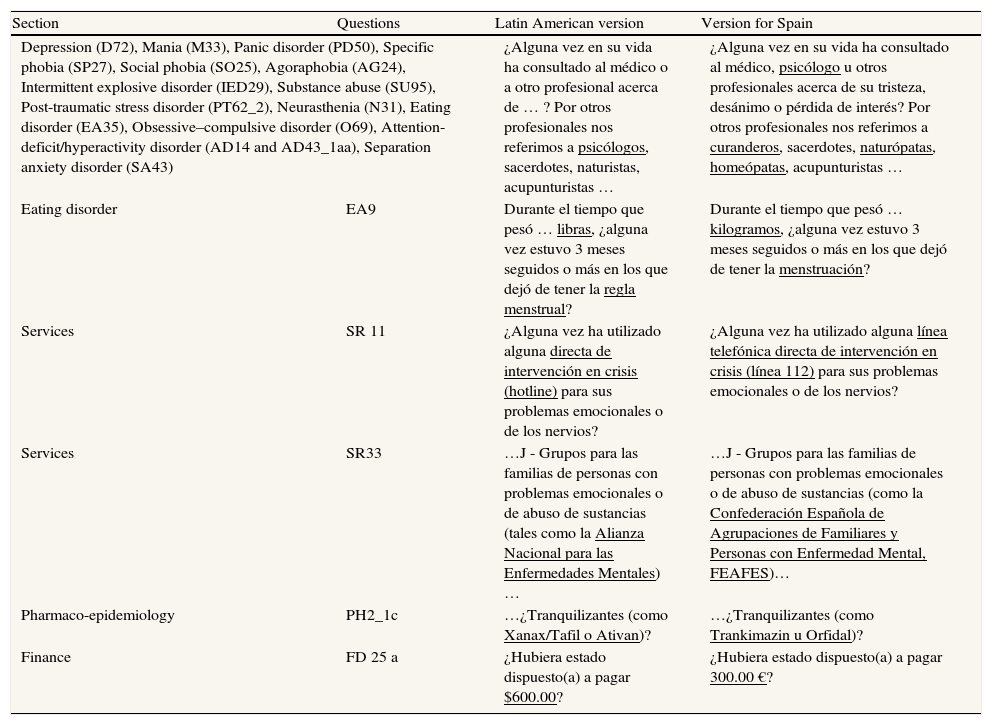
Other changes, including healthcare personnel designation, units of measurement and currency, names of Spanish institutions, organizations and psychotropic medication, as well as some other healthcare resources, also needed to be adapted for use in Spain (Table 4).
Examples of the adaptations related to health and economic resources introduced into the WHO-CIDI version for use in Spain.
| Section | Questions | Latin American version | Version for Spain |
| Depression (D72), Mania (M33), Panic disorder (PD50), Specific phobia (SP27), Social phobia (SO25), Agoraphobia (AG24), Intermittent explosive disorder (IED29), Substance abuse (SU95), Post-traumatic stress disorder (PT62_2), Neurasthenia (N31), Eating disorder (EA35), Obsessive–compulsive disorder (O69), Attention-deficit/hyperactivity disorder (AD14 and AD43_1aa), Separation anxiety disorder (SA43) | ¿Alguna vez en su vida ha consultado al médico o a otro profesional acerca de … ? Por otros profesionales nos referimos a psicólogos, sacerdotes, naturistas, acupunturistas … | ¿Alguna vez en su vida ha consultado al médico, psicólogo u otros profesionales acerca de su tristeza, desánimo o pérdida de interés? Por otros profesionales nos referimos a curanderos, sacerdotes, naturópatas, homeópatas, acupunturistas … | |
| Eating disorder | EA9 | Durante el tiempo que pesó … libras, ¿alguna vez estuvo 3 meses seguidos o más en los que dejó de tener la regla menstrual? | Durante el tiempo que pesó … kilogramos, ¿alguna vez estuvo 3 meses seguidos o más en los que dejó de tener la menstruación? |
| Services | SR 11 | ¿Alguna vez ha utilizado alguna directa de intervención en crisis (hotline) para sus problemas emocionales o de los nervios? | ¿Alguna vez ha utilizado alguna línea telefónica directa de intervención en crisis (línea 112) para sus problemas emocionales o de los nervios? |
| Services | SR33 | …J - Grupos para las familias de personas con problemas emocionales o de abuso de sustancias (tales como la Alianza Nacional para las Enfermedades Mentales)… | …J - Grupos para las familias de personas con problemas emocionales o de abuso de sustancias (como la Confederación Española de Agrupaciones de Familiares y Personas con Enfermedad Mental, FEAFES)… |
| Pharmaco-epidemiology | PH2_1c | …¿Tranquilizantes (como Xanax/Tafil o Ativan)? | …¿Tranquilizantes (como Trankimazin u Orfidal)? |
| Finance | FD 25 a | ¿Hubiera estado dispuesto(a) a pagar $600.00? | ¿Hubiera estado dispuesto(a) a pagar 300.00 €? |
Most of the 32 participants of the pilot study were males (66%), married or cohabiting (64.5%), with a mean age of 39 years (SD: 13.6), and a mean duration of formal education of 14 years (SD: 3.3). The median time to complete the entire interview was 2h and 10min with an interquartile range of between 1h 25min and almost 3h.
The correct functioning of the electronic adapted version (CAPI) was verified, specifically focusing on the complex skip out patterns of questions arising from the combination of answers previously given. Finally, after performing all the documentation necessary to reflect the changes made (Fig. 1), the adaptation of the LA versión of CIDI for Spain received official approval by the Editorial Committee of WMH-CIDI.
DiscussionThe CAPI format of the most current Latin American (v 20.0) Spanish version of the WHO-CIDI has been adapted following a rigorous and meticulous cross-cultural adaptation process and has been successfully pilot tested. It is over ten years since the last WHO-CIDI CAPI version was used in Spain and there have been many changes made during this time to improve the diagnostic interview and, therefore, to make it more relevant to present-day mental health availability and organization of services. However, this continuing process of up-dating the instrument has only been applied to the LA version which, because of cultural and linguistic factors, makes it unsuitable for use in Spain in its present form.
Although the questionnaire had already been translated into many languages, the last version specifically adapted for Spain was in the context of the ESEMeD project. During this time, the WHO-CIDI had gone through various iterations of improvement but the only currently available updated version was the LA CIDI (v. 20.0). We, therefore, used the most updated Spanish version of the CIDI available but only following the cultural and linguistic adaptation process described above.
The comprehensiveness and complexity of the instrument made the adaptation process particularly challenging, especially because of the interactive design of the diagnostic interview in the form of elaborate skip out patterns, complex randomization routines, question fills and edit checking during the course of the interview. This process results in the generation of questions which are directly linked to the answers previously provided by the interviewee. This, therefore, requires a very careful review of the CAPI version of the CIDI and a rigorous process of evaluation in the form of a pilot study.
The number of participants in the pilot study, included in the range previously suggested,17 was sufficient to activate and test all the survey sections to confirm their correct functioning and to allow an estimate of the administration time of the survey to be made. This administration time of the interview in our experience (2h and 10min approximately) was similar to that previously described in international studies.4 This time represents the median time for an interview when all the sections are answered. The administration time, however, can vary greatly depending on the number of diagnostic sections activated according to the pattern of positive responses answered by the interviewee in the initial screening section. In our case, the time ranged from a minimum of 54min to a maximum of 5h. The interactive design of the diagnostic interview allows the administration time of the interview to be shortened considerably for those interviewees who did not endorse symptoms of mental disorders in their lives and therefore respond negatively to many questions, but it can be very lengthy for those who respond affirmatively to a large number of questions in the screening interview. Moreover, the design also gives great flexibility to researchers to select the sections or modules to be activated depending on the study research questions. For example, certain research projects may wish to focus only on specific sections of the interview, depending on the topic under investigation, such as major depressive disorders. The CAPI format ensures maximum efficiency in terms of reducing the length of the interview as well as optimizing data management following completion of the interview.
The conventional cross-cultural adaptation process should be considered within a continuum, from one situation where no adaptation is needed as it is intended to be used in the same language and culture in which it was developed to the opposite pole in which the application of the questionnaire is to be used in a different culture, language and country.17,18 The situation outlined here falls somewhat in the middle (another country with the same language) so that no translation but only a cultural adaptation is needed. It is beyond the scope of this paper to completely assess all the psychometric characteristics of the CIDI (v. 3.0) for its use in Spain. As mentioned earlier, the process described here should be considered as part of the ongoing improvement process of continuous updating, refinement, validation and clinical calibration of the questionnaire led by the Editorial Committee of the WHO-CIDI.13–16,20
In summary, the CAPI format of the most current Latin American Spanish version of the CIDI has been adapted for use in Spain and its correct functioning has been successfully pilot tested. This version has been successfully tested and received official approval, so that it can now be widely employed for further mental health epidemiological studies in Spain.
The World Health Organization Composite International Diagnostic Interview (WHO-CIDI) was designed by the WHO for the purpose of ascertaining diagnoses in epidemiological studies of mental illnesses in the general population to allow cross-national comparative research. The WHO-CIDI is a highly structured interview that has been widely translated to several languages. The current CIDI Latin American version needs a cultural adaptation process to be used in Spain due to linguistic and cultural differences.
What is new?The CAPI format of the WHO-CIDI has been successfully adapted and its correct functioning has been pilot-tested for its use in Spain following a predetermined protocol supervised by the Editorial Committee of the instrument. This version will facilitate the use of an international diagnostic instrument allowing cross-national comparative research in the new epidemiological studies of mental illnesses in Spain.
M.J. Tormo, J. Alonso, S. Aguilar-Gaxiola, C. Navarro and F. Navarro-Mateu conceived the design and supervised the whole process of the study. I. Morán-Sánchez, F. Navarro-Mateu, M.L. Pujalte and A. Garriga were, simultaneously, accredited as trainers for future interviewers. I. Morán-Sánchez, M.L. Pujalte, A. Garriga, J. Alonso, M.J. Tormo, S. Aguilar-Gaxiola and F. Navarro-Mateu participated in the adaptation process. All authors read, edited and approved the final manuscript.
FundingThis work has been financed by the Murcian Health Service, the Cajamurcia Foundation and the Foundation for Healthcare Training and Research (FFIS) of the Murcia Region.
Conflict of interestNone.
We thank Carlos Giribert Muñoz, Deputy Sub-Director of Mental Health and Psychiatric Services, Murcia Health Service, for his support in developing the PEGASUS-Murcia project; Guadalupe Ruiz Merino and David Martínez, from the Foundation for Healthcare Training and Research (Fundación para la Formación e Investigación Sanitarias, FFIS) of the Murcia Region, for their collaboration in the adaptation process; Javier Júdez, Salvador Martínez and Gemma Villagut for their collaboration in the PEGASUS-Murcia project; Corina Benjet and Jerónimo Blanco for their support as expert trainers during the WHO-CIDI training; and Mike Tobin for his helpful discussions and contribution during the English translation of the document.









