


The objective of the prospective cohort study (the DESKcohort project) is to describe and monitor health, health behaviors, and their related factors among 12 and 19-year-old adolescents schooled at centers of Compulsory Secondary Education or post-compulsory secondary education in Central Catalonia, considering social determinants of health. The DESKcohort survey is administered biannually between the months of October and June, and the project has been running for three years. We have interviewed 7319 and 9265 adolescents in the academic years 2019/20 and 2021/22, respectively. They responded a questionnaire created by a committee of experts, that included the following variables: sociodemographic factors, physical and mental health, food, physical activity, leisure and mobility, substance use, interpersonal relationships, sexuality, screen use and digital entertainment, and gambling. The results are presented to educational centers, county councils, municipalities, and health and third sector entities to plan, implement, and evaluate prevention and health promotion actions that address the identified needs.
El objetivo de este estudio prospectivo de cohortes (proyecto DESKcohort) es describir y monitorizar la salud, los comportamientos de salud y sus factores asociados en los adolescentes de entre 12 y 19 años escolarizados en centros de Educación Secundaria Obligatoria o secundaria posobligatoria de la Cataluña Central, considerando los determinantes sociales de la salud. La encuesta DESKcohort se realiza bianualmente, entre los meses de octubre y junio, y el proyecto lleva 3 años en marcha. Se ha entrevistado a 7319 y 9265 adolescentes en los cursos 2019/20 y 2021/22, respectivamente. Respondieron un cuestionario creado por un comité de expertos, que incluía las siguientes variables: sociodemográficas, salud física y mental, alimentación, actividad física, ocio y movilidad, consumo de sustancias, relaciones interpersonales, sexualidad, uso de pantallas y entretenimiento digital, y juegos de azar. Los resultados son presentados a los centros educativos, las diputaciones, los municipios y las entidades sanitarias y del tercer sector para planificar, implementar y evaluar acciones de prevención y promoción de la salud que aborden las necesidades identificadas.
Adolescence is characterized by risk-taking and experimentation of new environments and behaviors, and health habits developed during this period have an impact on long-term health and well-being.1,2 These behaviors, such as alcohol consumption or tobacco use, are not only related to individual factors, but also to social factors.3-5
However, adolescents have the potential for successful and healthy development because human development is not predefined.6 In this sense, it is important to collect information on the health status of the population and its determinants.7 Although health behavior monitoring tools for young people have been used over the years, they have mostly focused in urban populations.8 However, in rural environments, the social, demographic, and geographic characteristics are distinct, and adolescents behave differently from their peers in urban areas.9 In this context, there is a need to create a surveillance system to monitor health behaviors and their determinants among adolescents in rural settings. Also, health behaviors are mostly investigated through cross-sectional surveys; therefore, it is important to implement longitudinal studies to analyze current health behaviors, how they change in the same adolescents, and their determinants over time. As proposed, in order to carry out a good surveillance of the determinants of health, the social determinants of health must be taken into account.7 The conceptual framework of reference is the Conceptual Framework of the determinants of social inequalities in health of the Commission for the Reduction of Health Inequalities in Spain.
The objective of the prospective cohort study (the DESKcohort project) is to describe and monitor health, health behaviors, and their related factors among 12 and 19-year-old adolescents schooled at centers of Compulsory Secondary Education or post-compulsory secondary education in Central Catalonia (Spain), considering social determinants of health.
MethodThe Determinants of Health in Secondary School Students in Central Catalonia (DESKcohort) project is a prospective longitudinal study with successive waves that provide comparable cross-sectional information and allow longitudinal assessment of changes in health behaviors (see table I in online Appendix). Participants are interviewed biannually (Table 1), creating a cohort of adolescents. To link students from one wave to the next and do a follow-up, a unique identifier was created for each student.
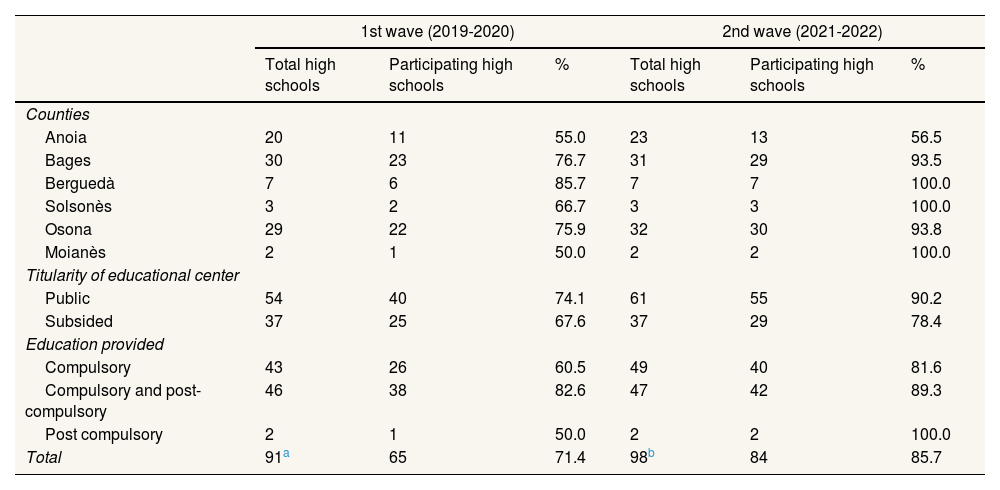
Distribution of educational centers and total participation by region, titularity of the educational center and level of education provided in the 1st and 2nd wave of DESKcohort project.
| 1st wave (2019-2020) | 2nd wave (2021-2022) | |||||
|---|---|---|---|---|---|---|
| Total high schools | Participating high schools | % | Total high schools | Participating high schools | % | |
| Counties | ||||||
| Anoia | 20 | 11 | 55.0 | 23 | 13 | 56.5 |
| Bages | 30 | 23 | 76.7 | 31 | 29 | 93.5 |
| Berguedà | 7 | 6 | 85.7 | 7 | 7 | 100.0 |
| Solsonès | 3 | 2 | 66.7 | 3 | 3 | 100.0 |
| Osona | 29 | 22 | 75.9 | 32 | 30 | 93.8 |
| Moianès | 2 | 1 | 50.0 | 2 | 2 | 100.0 |
| Titularity of educational center | ||||||
| Public | 54 | 40 | 74.1 | 61 | 55 | 90.2 |
| Subsided | 37 | 25 | 67.6 | 37 | 29 | 78.4 |
| Education provided | ||||||
| Compulsory | 43 | 26 | 60.5 | 49 | 40 | 81.6 |
| Compulsory and post-compulsory | 46 | 38 | 82.6 | 47 | 42 | 89.3 |
| Post compulsory | 2 | 1 | 50.0 | 2 | 2 | 100.0 |
| Total | 91a | 65 | 71.4 | 98b | 84 | 85.7 |
The geographical scope of the survey is Central Catalonia, which comprises the counties of Anoia, Bages, Berguedà, Moianès, Osona, and Solsonès, including 165 of the 947 municipalities in Catalonia. In this territory, there are currently 96 educational centers of Compulsory Secondary Education and two centers of post-compulsory education (baccalaureate and formative cycles). The study population consists of students in 2nd and 4th of compulsory secondary education (CSE); 2nd of post-compulsory secondary education (PCSE); and 2nd of Intermediate Level Training Cycles (ILTC). The DESKcohort project is a collaborative project led by the Fundació Universitària del Bages (FUB) with the participation of the Subdirectorate General for Addictions, HIV, Sexually Transmitted Infections and Viral Hepatitis; the Departament d’Educació; the Centre d’Estudis Epidemiològics sobre el VIH/SIDA de Catalunya (CEEISCAT); the Universitat Oberta de Catalunya (UOC); the Autonomous University of Barcelona; the Universidad de Alicante (UA); and the Consorcio de Investigación Biomédica en Red de Epidemiología y Salud Pública (CIBERESP).
Participant recruitmentBefore the end of the academic year and prior to data collection (around May-June), we send a letter to all educational centers in the region to invite them to participate in the project. To the ones agreeing to participate, we also send informed consent forms to be signed by the adolescents’ legal guardians. Adolescents over 14 years of age can sign the informed consent themselves, according to the Spanish Official Personal Data Protection Act. Then, at the beginning of the academic year in which the data collection will take place (September), we contact the schools to schedule a date for administering the questionnaire.
Data collection tools and proceduresThe initial DESKcohort questionnaire was elaborated by was prepared by researchers from the University of Bages Foundation, the Open University of Catalonia, the CEEISCAT and the Public Health Agency of Catalonia on the basis of other questionnaires on health behaviors during adolescence8,10-12 with high validity and reliability, from studies with a long track record (see table II in online Appendix).13-16 The successive versions were produced by the scientific committee (http://deskcohort.cat/en/scientific-committee/). The questionnaire had different sections: sociodemographic factors, physical and mental health, food, physical activity, leisure and mobility, substance use, interpersonal relationships, sexuality, screen use and digital entertainment, and gambling (see table I in online Appendix). The scientific committee meets every year to review the questionnaire and decide whether to add a section with new questions or the required improvements between waves. For example, in the 2020/21 academic year, questions on COVID-19 were introduced.
Data collection is performed biannually between the months of October and June, corresponding to the academic calendar of the Catalan educational system (1st wave in the academic year 2019-20; 2nd wave in the academic year 2021-22). The questionnaire is online and self-administered in the classrooms. It is built with the Redcap (Research Electronic Data Capture) software.17 Of the students in the 2nd year of ESO and 4th year of ESO, 46.7% were followed.
Ethical aspectsThe project was approved by the Ethics Committee of the Universitat de Vic-Universitat Central de Catalunya (UVic-UCC) (96/2019). All the information is stored online in a secure server of the Fundació Universitària del Bages, guaranteeing confidentiality according to the Official Personal Data Protection Act. Data with identification codes are dissociated from the responses to the questionnaire, and only the principal investigator has access to the database with the identification codes.
Data analysisTo analyse the data in the cross-sectional and longitudinal studies we will calculate the prevalence and cumulative incidences of the health conditions or behaviours to be studied, respectively. These prevalence and incidence will be calculated for the total and for each category of the different independent variables. To analyse the relationship between both proportions and the different independent variables we will estimate Poisson regression models with Robust variance obtaining Prevalence Ratios or Relative Risks with their respective 95% confidence intervals.18 All the analyses were performed using STATA17 software.
ResultsSixty-five (71.4%) and 84 (85.7%) centers have participated in the first and second waves, respectively. Table 1 describes the participation rate in each county. In the first wave, 7319 adolescents out of 11943 have participated (61.3%), and in the second wave, 9265 out of 14342 (64.6%). Table 2 describes the characteristics of the participants in the two waves of the DESKcohort project, in terms of sex, course grade, self-reported socioeconomic level, region of residence, and type of educational center (public or private). In the second wave, the prevalence of risky behaviors was higher than in the previous one; in both waves we generally observe that girls have engaged more in less healthy behaviors than boys. Of the 2505 people followed between the 1st and the follow-up period, 56.0% are girls. Also, within the cohort, 56.1% of people have been followed from 2nd to 4th year of CSE, 43.6% from 4th year of CSE to 2nd year of PCSE or 2nd year of ILTC. Therefore, we have included a table (see table III in online Appendix) detailing the sociodemographic characteristics of the people who in the first wave were likely to be followed up in the second wave, and the people who are followed up in the 2nd wave.
Description of the sample prevalence of the main health behaviors, from the 1st and 2nd waves of DESKcohort study and stratified by sex.
| Boys | Girls | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1st wave | 2nd wave | 1st wave | 2nd wave | |||||||||
| n | % | CI95% | n | % | CI95% | n | % | CI95% | n | % | CI95% | |
| Total | 3505 | 47.9 | 46.8-49.0 | 4558 | 49.2 | 48.2-50.2 | 3814 | 52.1 | 50.9-53.3 | 4707 | 50.8 | 49.8-51.8 |
| Region of residence | ||||||||||||
| Anoia | 660 | 18.8 | 17.6-20.2 | 752 | 16.5 | 15.4-17.6 | 767 | 20.1 | 18.9-21.4 | 731 | 15.5 | 14.5-16.6 |
| Bages | 1226 | 35.0 | 33.4-36.6 | 1497 | 32.8 | 31.5-34.2 | 1277 | 33.5 | 32.0-35.0 | 1651 | 35.1 | 33.7-36.5 |
| Berguedà | 324 | 9.2 | 8.3-10.2 | 392 | 8.6 | 7.8-9.4 | 304 | 8.0 | 7.2- 8.9 | 347 | 7.4 | 6.7-8.2 |
| Solsonès | 46 | 1.3 | 1.0- 1.7 | 87 | 1.9 | 1.5-2.3 | 69 | 1.8 | 1.4- 2.3 | 79 | 1.7 | 1.3-2.1 |
| Moianès | 81 | 2.3 | 1.9- 2.9 | 156 | 3.4 | 2.9-4.0 | 117 | 3.1 | 2.6- 3.7 | 169 | 3.6 | 3.1-4.2 |
| Osona | 1087 | 31.0 | 29.5-32.6 | 1581 | 34.7 | 33.3-36.1 | 1173 | 30.8 | 29.3-32.2 | 1623 | 34.5 | 33.1-35.9 |
| Othersa | 81 | 2.3 | 1.9- 2.9 | 93 | 2.0 | 1.7-2.5 | 107 | 2.8 | 2.3- 3.4 | 107 | 2.3 | 1.9-2.7 |
| Courseb | ||||||||||||
| 2nd CSE | 1296 | 37.0 | 35.4-38.6 | 1458 | 32.0 | 30.6-33.4 | 1382 | 36.2 | 34.7-37.8 | 1428 | 30.3 | 29.0-31.7 |
| 4th CSE | 1316 | 37.5 | 36.0-39.2 | 1752 | 38.4 | 37.0-39.9 | 1374 | 36.0 | 34.5-37.6 | 1773 | 37.7 | 36.3-39.1 |
| 2nd PCSE | 649 | 18.5 | 17.3-19.8 | 883 | 19.4 | 18.3-20.5 | 863 | 22.6 | 21.3-24.0 | 1203 | 25.6 | 24.3-26.8 |
| 2nd ILTC | 244 | 7.0 | 6.2- 7.9 | 465 | 10.2 | 9.4-11.1 | 195 | 5.1 | 4.5- 5.9 | 303 | 6.4 | 5.8-7.2 |
| Type of schoolc | ||||||||||||
| Subsided | 1087 | 31.0 | 29.5-32.6 | 1398 | 30.7 | 29.3-32.0 | 994 | 26.1 | 24.7-27.5 | 1301 | 27.6 | 26.4-28.9 |
| Public | 2418 | 69.0 | 67.4-70.5 | 3160 | 69.3 | 68.0-70.7 | 2820 | 73.9 | 72.5-75.3 | 3406 | 72.4 | 71.1-73.6 |
| Socioeconomic positiond | ||||||||||||
| Lower | 1221 | 34.8 | 33.3-36.4 | 1581 | 34.7 | 33.3-36.1 | 1375 | 36.1 | 34.5-37.6 | 1657 | 35.2 | 33.9-36.6 |
| Medium | 1180 | 33.7 | 32.1-35.2 | 1533 | 33.6 | 32.3-35.0 | 1239 | 32.5 | 31.0-34.0 | 1512 | 32.1 | 30.8-33.5 |
| High | 1104 | 31.5 | 30.0-33.1 | 1444 | 31.7 | 30.3-33.0 | 1200 | 31.5 | 30.0-33.0 | 1538 | 32.7 | 31.3-34.0 |
| Self-perceived health | ||||||||||||
| Excellent or very good | 2290 | 65.3 | 63.7-66.9 | 3206 | 70.3 | 69.0-71.6 | 1911 | 50.1 | 48.5-51.7 | 2292 | 48.7 | 47.3-50.1 |
| Good, fair or poor | 1215 | 34.7 | 33.1-36.3 | 1352 | 29.7 | 28.4-31.0 | 1903 | 49.9 | 48.3-51.5 | 2415 | 51.3 | 49.9-52.7 |
| State of mind | ||||||||||||
| Good mood | 3075 | 87.7 | 86.6-88.8 | 3789 | 83.1 | 82.0-84.2 | 2829 | 74.1 | 72.8-75.5 | 2734 | 58.1 | 56.7-59.5 |
| Low mood | 430 | 12.3 | 11.2-13.4 | 769 | 16.9 | 15.8-18.0 | 985 | 25.8 | 24.5-27.2 | 1973 | 41.9 | 40.5-43.3 |
| Spanish Healthy Eating Index | ||||||||||||
| Health | 186 | 5.3 | 4.6- 6.1 | 353 | 7.7 | 7.0- 8.6 | 416 | 10.9 | 10.0-11.9 | 658 | 14.0 | 13.0-15.0 |
| Needs changes | 3070 | 87.6 | 86.5-88.6 | 3800 | 83.4 | 82.3-84.4 | 3168 | 83.1 | 81.8-84.2 | 3671 | 78.0 | 76.8-79.2 |
| Unhealthy | 249 | 7.1 | 6.3- 8.0 | 405 | 8.9 | 8.1- 9.7 | 230 | 6.0 | 5.3- 6.8 | 378 | 8.0 | 7.3- 8.8 |
| Physical activitye | ||||||||||||
| Comply WHO | 1968 | 60.0 | 58.3-61.7 | 2615 | 60.9 | 59.4-62.3 | 1303 | 37.2 | 35.6-38.8 | 1752 | 38.8 | 37.4-40.2 |
| Not complying WHO | 1310 | 40.0 | 38.3-41.7 | 1682 | 39.1 | 37.7-40.6 | 2200 | 62.8 | 61.2-64.4 | 2762 | 61.2 | 59.8-62.6 |
| Daily smoking tobacco | ||||||||||||
| No | 3271 | 93.3 | 92.4-94.1 | 4308 | 94.5 | 93.8-95.1 | 3497 | 91.7 | 90.8-92.5 | 4330 | 92.0 | 91.2-92.7 |
| Yes | 234 | 6.7 | 5.9- 7.6 | 250 | 5.5 | 4.9- 6.2 | 317 | 8.3 | 7.5- 9.2 | 377 | 8.0 | 7.3- 8.8 |
| Hazardous drinkingf | ||||||||||||
| No | 2691 | 76.8 | 75.3-78.1 | 3379 | 74.1 | 72.8-75.4 | 2869 | 75.2 | 73.8-76.6 | 3390 | 72.0 | 70.7-73.3 |
| Yes | 814 | 23.2 | 21.9-24.7 | 1179 | 25.9 | 24.6-27.2 | 945 | 24.8 | 23.4-26.2 | 1317 | 28.0 | 26.7-29.3 |
| Hazardous cannabis consumptiong | ||||||||||||
| No | 3355 | 95.7 | 95.0-96.3 | 4426 | 97.1 | 96.6-97.6 | 3677 | 96.4 | 95.8-97.0 | 4576 | 97.2 | 96.7-97.7 |
| Yes | 150 | 4.3 | 3.7- 5.0 | 132 | 2.9 | 2.4- 3.4 | 137 | 3.6 | 3.0- 4.2 | 131 | 2.8 | 2.3- 3.3 |
| Having suffered bullying | ||||||||||||
| No | 3064 | 91.2 | 90.2-92.1 | 3901 | 85.6 | 84.5-86.6 | 3349 | 92.6 | 91.7-93.4 | 3804 | 80.8 | 79.7-81.9 |
| Yes | 296 | 8.8 | 7.9- 9.8 | 657 | 14.4 | 13.4-15.5 | 268 | 7.4 | 6.6- 8.3 | 903 | 19.2 | 18.1-20.3 |
| Condom use | ||||||||||||
| Yes | 446 | 70.2 | 66.6-73.7 | 412 | 53.6 | 50.1-57.2 | 501 | 61.9 | 58.5-65.2 | 458 | 46.0 | 42.9-49.1 |
| No | 189 | 29.8 | 26.3-33.4 | 356 | 46.4 | 42.8-49.9 | 308 | 38.1 | 34.8-41.5 | 538 | 54.0 | 50.9-57.1 |
| Betting | ||||||||||||
| No | 313 | 86.9 | 83.0-90.1 | 3989 | 88.4 | 87.5-89.3 | 415 | 91.6 | 88.7-93.8 | 4439 | 95.1 | 94.4-95.7 |
| Yes | 47 | 13.1 | 9.9-17.0 | 522 | 11.6 | 10.7-12.5 | 38 | 8.4 | 6.2-11.3 | 229 | 4.9 | 4.3- 5.6 |
CSE: Compulsory Secondary Education; ILTC: Intermediate Level Training Cycles; PCSE: Post-Compulsory Secondary Education; WHO: World Health Organization.
The “Others” category includes those people who live in a region that does not belong to the territory of Central Catalonia.
Self-reported data recorded from the question of the DESKcohort questionnaire “What course do you go to?”.
Self-reported data recorded from the question of the DESKcohort questionnaire “Which high school do you go to?”. The Departament d’Educació de la Generalitat de Catalunya provides the data on the ownership of the educational centers of Central Catalonia updated annually, and from them the researchers create this variable by assigning the type of school of the educational center to each participating institute.
Terciles obtained from McArthur Scale results, which inquired for neighborhood self-perceived socioeconomic position.
Young people have different health-related behaviors from adults, but there are few data about youth health needs over the years. The DESKcohort project contributes to the characterization of health behaviors and their changes throughout adolescence and studies the determinants of these changes. Our initial descriptive results indicate that with age, behaviors become less healthy in terms of mental health, wellbeing, physical activity, and diet; and risky behaviors like problematic use of addictive substances increase. Several scientific papers have already been published with DESK data. They have estimated poly-consumption of cannabis and tobacco,19 found socio-economic differences in nutrition during COVID-19 confinement,20 found social inequalities in skipping breakfast21 and reported a decrease in substance use during COVID-1922 confinement as well as changes in their mental health and social conditions.23,24 So, it is important to identify in what groups and at what ages these changes occur and to detect risk factors to promote healthy behaviors and prevent risky behaviors at later stages.
The DESKcohort is expected to be a leading monitoring project in Catalonia. Between the 1st and 2nd waves, the participation increased by 14.3%, and it is expected to continue increasing in the successive ones. This will allow to increase the sample size, increase variability of the sample, and make more accurate inferences on the population.
DiscussionDuring the first three years of the DESKcohort project, data from 7319 and 9265 students in Central Catalonia have been analyzed for the 2019/20 and 2021/22 school years, respectively. Specifically, we performed a descriptive cross-sectional analysis and an analytic longitudinal analysis of the health behaviors of students in 2nd and 4th year of CSE, 2nd year of PCSE, and 2nd year of ILTC.
One limitation of this project is the exclusion of adolescents outside the formal educational system; therefore, the representativeness of the sample is limited to students enrolled in educational centers of the territory. However, education in our country is compulsory until the age of 16; therefore, this limitation would be relevant only for adolescents in the 2nd year of post-compulsory secondary education, a fact that is minimized by including adolescents in the 2nd year of ILTC. Another limitation is that not all educational centers invited to participate did participate in the end. Moreover, nor all students in the participating educational centers responded to the questionnaire. However, in five of the six counties, in the 2nd wave over 90% of the educational centers decided to participate in the study (Table 1). The fact that participation may vary in each wave makes it difficult to establish a stable cohort that monitors individuals from 2nd year of CSE to 2nd year of PCSE or 2nd year of ILTC. This can lead to a low follow-up rate throughout the entire academic trajectory, and individuals are followed intermittently without sustained progress. Finally, responses to the questionnaire are self-reported and data could suffer some information bias (for example, because of social desirability and recall bias). However, the questionnaire included questions with a high validity for adolescents: for example, CAST and AUDIT-C13,25 in the case of substance use; and other tests in the case of bullying, mental health, and problematic screen use26-29.
As a strength of the DESKcohort project, we highlight the importance for the region to have monitoring data on the health behaviors of adolescents, and to be able to analyze the effect of contextual factors and social determinants on them, besides the high participation rate and sample size. Also, after each wave, we returned the results to participating educational centers and regional institutions. This allows the educational centers to detect and identify health needs to implement programs adapted to these needs among their students. In addition, a general results report is published biannually, which allows the identification of the health needs of the population. Finally, as a longitudinal monitoring tool, the DESKcohort project complements other information systems to understand health and its determinants among adolescents in Catalonia. It represents a crucial source of information for both local (educational centers, county councils, municipalities, and health and third sector entities) and national policy making institutions (Health Department, Education Department). This allows them to improve health promotion strategies and public health programs to address the identified needs and evaluate future interventions.
Availability of databases and material for replicationData collected and generated in the DESKcohort project are available free of charge for scientific research. Following the data cleaning, processing and the generation variables of each wave, people can ask for obtain some modules of variables. To obtain data, researchers could be addressed DESKcohort website (http://deskcohort.cat/en/databases/). Then, DESKcohort checks the purpose of the request and the affiliation of the applicant and provides the database, always without the identification code data created. As of January 2023, data from the first waves 1 and 2 are available (transversal and longitudinal data).
Editor in chargeMariano Hernán-García.
Authorship contributionsA. Espelt is the principal investigator of the DESKcohort project, and he conceived and led the preparation of the research protocol. M. Bosque-Prous, E. Teixidó-Compañó, C. Folch, J. Colom, J. Casabona, C. Vives-Cases and E. Fernandez reviewed and proposed questions from their respective areas of expertise to be included in the DESKcohort questionnaire. J. Rogés, M. Bosque-Prous, H. González-Casals, G. Drou, E. Teixidó-Compañó and A. Espelt collected the data. J. Rogés, H. González-Casals, G. Drou and A. Espelt performed the data analysis, interpretation of the results and creation of the tables. J. Rogés drafted the article. A. Espelt and M. Bosque-Prous reviewed the structure and design of the manuscript. All the coauthors discussed, reviewed and approved the manuscript in its last version, and made important contributions from their field of expertise that contributed to enriching the manuscript.
The authors wish to thank the educational centers that agreed to collaborate with the project and all the students that participated in the study. We are also thankful for the support of the Departament de Salut and the Departament d’Educació de la Generalitat de Catalunya. Additionally, authors are thankful to CERCA Programme/Generalitat de Catalunya for institutional support. Finally, we want to acknowledge the DESK-Cohort Project Working Group (in alphabetical order): Aguilar, Alicia; Àlvarez, Anaís; Angulo-Brunet, Ariadna; Arechavala, Teresa; Baena, Antoni; Barón-García, Tivy; Bartroli, Montse; Borao, Olga; Caberol, Ariadna; Campoy, Mireia; Clotas, Catrina; Colillas-Malet, Ester; Díaz-Geada, Ainara; Espino, Sandra; Esquius, Laura; Gontié, Rémi; Jubany, Júlia; Majó, Xavier; Manera, Maria; Munné, Carles; Muntaner, Carles; Obradors-Rial, Núria; Puigcorbé, Susanna; Riera, Carlota; Saigí, Francesc; Torralba, Mireia; Torruella, Anna; Vaqué, Cristina.
This paper is part of the doctoral Dissertation of J. Rogés at the Universitat Oberta de Catalunya.









