

To determine differences between men and women in hazardous drinking, heavy cannabis use and hypnosedative use according to educational level and employment status in the economically active population in Spain.
MethodCross-sectional study with data from 2013 Spanish Household Survey on Alcohol and Drugs on individuals aged 25-64 [n=14,113 (women=6,171; men=7,942)]. Dependent variables were hazardous drinking, heavy cannabis use and hypnosedative consumption; the main independent variables were educational level and employment situation. Associations between dependent and independent variables were calculated with Poisson regression models with robust variance. All analyses were stratified by sex.
ResultsHazardous drinking and heavy cannabis use were higher in men, while women consumed more hypnosedatives. The lower the educational level, the greater the gender differences in the prevalence of this substances owing to different consumption patterns in men and women. While men with a lower educational level were higher hazardous drinkers [RII=2.57 (95%CI: 1.75-3.78)] and heavy cannabis users [RII=3.03 (95%CI: 1.88-4.89)] compared to higher educational level, in women the prevalence was the same. Women with a lower education level and men with a higher education level had higher hypnosedative consumption. Unemployment was associated with increased heavy cannabis use and hypnosedative use in both women and men and with lower hazardous drinking only in women.
ConclusionsThere are differences between men and women in the use of psychoactive substances that can be explained by the unequal distribution of substance use in them according to educational level. Unemployment was associated with substance use in both men and women.
Determinar las diferencias entre hombres y mujeres en cuanto a consumo de riesgo de alcohol, de cánnabis y en el consumo de hipnosedantes según el nivel educativo y la situación laboral en la población activa española.
MétodosEstudio transversal con datos de la Encuesta Domiciliaria sobre Alcohol y Drogas en España (2013) de personas de 25-64 años de edad (n=14.113 [mujeres=6.171; hombres=7.942]). Las variables dependientes fueron consumo de riesgo de alcohol, consumo de cánnabis y consumo de hipnosedantes; las principales independientes fueron el nivel de estudios y la situación laboral. Para estimar la asociación entre variables dependientes e independientes se calcularon modelos de regresión de Poisson con varianza robusta. Todos los análisis se estratificaron por sexo.
ResultadosLos hombres tenían mayor consumo de riesgo de alcohol y cánnabis, mientras que las mujeres consumían más hipnosedantes. A menor nivel de estudios, mayores diferencias de sexo en el consumo de estas sustancias. Esto fue debido al patrón distinto de mujeres y hombres. Mientras los hombres con un menor nivel de estudios tenían mayor consumo de riesgo de alcohol (RII=2,57; IC95%: 1,75-3,78) y cánnabis (RII=3,03; IC95%: 1,88-4,89), en comparación con los de un mayor nivel de estudios, la prevalencia en las mujeres era la misma. Las mujeres con menor nivel de estudios y los hombres con mayor nivel de estudios consumían más hipnosedantes. La desocupación se asociaba a un mayor consumo de riesgo de cánnabis y de hipnosedantes tanto en las mujeres como en los hombres, y a un menor consumo de riesgo de alcohol solo en las mujeres.
ConclusionesExisten diferencias entre los hombres y las mujeres en el consumo de sustancias psicoactivas. Estas diferencias pueden explicarse por la desigual distribución del consumo de sustancias en ambos sexos según el nivel de estudios. La desocupación se asociaba al consumo de sustancias tanto en los hombres como en las mujeres.
Different social conditions and power relationship between women and men can affect and/or condition behaviours1 such as substance use. The prevalence of hazardous drinking or heavy cannabis use at both European and country level is greater in men than in women.2–5 Conversely, the prevalence of psychotropic drug use, such as hypnotics or sedatives, is higher in women.4,6–8 Drug consumption is also related to living conditions, access to economic resources or employment status.9 It has been reported that people with worse living conditions may be exposed to more stressful situations that could lead to detrimental health behaviours.9 In developed countries, an association between educational level and alcohol,5,10,11 cannabis12 and hypnosedative use6 has been found. In addition, employment status is associated with substance use, both licit and illicit, and even with substance dependence.10,13,14 The mechanisms that might explain the previous associations are various and sometimes contradictory.4,15 For example, substance use could increase in adverse social conditions as a means to cope with psychological distress, or may decrease due to the lack of financial resources. Besides, we can not rule out an inverse relationship, since it has been found that substance use during adolescence is associated with lower education and worse employment outcomes in adulthood.16
Regardless of the direction of the association, the relationship between educational level or employment status and substance use could vary between men and women. In Europe, while higher prevalence of hazardous drinking is found in men with lower education level, among women, the highest prevalence is found in those with higher education level.11,17 However, a recent study in Spain shows that hazardous drinking increases with the education level in both, women and men.5 Besides, some studies show that the association between unemployment and substance use is stronger in men than women,4,13 whereas others report the opposite.17 The study of the differences between men and women in substance use is especially relevant in a period of economic crisis. In Spain the crisis has led to an increase in mental health problems in men, due to their unemployment,18 and an increase in substance abuse, especially of alcohol and hypnosedatives in both women and men, regardless of their employment status, and cannabis only in unemployed men.4 In fact, in a period of crisis, job loss could be a predictor of becoming a hazardous drinker.14 However, although there are studies aimed at analysing the relationship between educational level and employment status and their influence on health in Spain, we are not aware of the existence of studies that specifically analyse the differences between men and women in substance use in relation to educational level and employment status.
This study aims to: 1) describe the differences in the prevalence of hazardous drinking, heavy cannabis use and hypnosedative consumption between economically active men and women aged 25 to 64 resident in Spain by educational level and employment status, and 2) analyse how educational level and employment status are related with the consumption of these psychoactive substances in economically active women and men.
MethodsThis is a cross-sectional study with data from the Spanish Household Survey on Alcohol and Drugs (EDADES) from 2013 (the last edition accessible by the Government Delegation for the National Plan on Drugs: www.pnsd.msssi.gob.es). EDADES is a national survey with a representative sample of the non-institutionalised Spanish population aged 15 to 64 years. Data collection was performed through face-to-face interviews with two questionnaires: one about sociodemographic variables (conducted by an interviewer) and the other about substance use variables (self-administered). A tri-stage clustered probability without substitution was employed, oversizing the initial sample to cover the unrealizable interviews. For this study, we included people, currently working or unemployed at the time of the survey, excluding people younger than 25 years, to assure that they could have attained the highest level of education (university), and the economically inactive individuals (students, homemakers, retired, disabled).4 We also excluded those who had not answered some questions about alcohol, cannabis or hypnosedatives and all people without information for any of the independent variables included in the study (less than 4%). Likewise, sample weights were applied to ensure representativeness. The final sample consisted of 14,113 individuals.
Variables- 1)
Dependent variables:
Hazardous drinking was constructed based on the Alcohol Use Disorders Identification Test (AUDIT), a screening validated test developed by the World Health Organisation (WHO). The AUDIT consists in 10 questions scored from 0 to 4 about recent alcohol use, alcohol dependence symptoms and alcohol-related problems, and the final sum allows to identify persons with hazardous drinking and alcohol-use disorders.19 In men, hazardous drinking was considered when the total sum was 8 or more, and in women, when was 6 or more.20
Heavy cannabis use was determined from the Cannabis Abuse Screening Test (CAST), a validated test that screens for different aspects of harmful cannabis use by assessing the frequency of different events within the last 12 months.21 The CAST consists in 6 items, scored from 0 to 4, which identify patterns or risky behaviors related to cannabis use. Heavy cannabis use was considered when the sum was 7 or more.21
Hypnosedative consumption was based on the consumption of tranquilizers, sedatives or sleeping pills over the last twelve months, regardless of whether they were prescribed or not.4 The questionnaire clarified that they were pills to calm nerves or anxiety (tranquilizers, sedatives) or to sleep (sleeping pills).
- 2)
Independent variables:
The main independent variables were educational level, employment status and sex (women; men). Educational level was used as a proxy of SEP, as proposed elsewhere,22,23 since it can be applied to unemployed people and is stable over the adult lifespan. Educational level was obtained through the question “Which is the highest level of studies you have completed?”, and collapsing the six possible response options into three categories [primary education or lower; secondary education; higher education]. Employment status was constructed from the question “Which of the following best describes your situation during the past week?”, classifying people as employed or unemployed. Other variables analysed were age, marital status, Spanish region of residence and self-perceived health.
All the analyses were performed separately for women and men. The prevalence of hazardous drinking, heavy cannabis use and hypnosedative consumption was estimated by educational level and employment status with their respective 95% confidence intervals (95%CI). To analyse whether there were sex differences in the prevalence of substance use in each one of the educational level and employment status categories, prevalence ratios (PR) were calculated between men and women adjusting for the other independent variables. To estimate associations of hazardous drinking, heavy cannabis use and hypnosedative consumption with educational level and employment status, Poisson regression models with robust variance were fitted, obtaining a PR with a 95%CI.24 For educational level we calculated the Relative Index of Inequality (RII). This required previous conversion of the educational level variable to a scale variable (values from 0 to 1) measuring, for each category, the cumulative proportion of the population that has a lower position in the hierarchy. For each dependent variable, two different models were estimated. In the first model, both the educational level and employment status were introduced in the model. The second included the possible modifying effect of the independent variables. If the interaction between educational level and employment status in the second model was not statistically significant, the first model was considered the most suitable. All the models were adjusted for age, marital status, Spanish region of residence and self-perceived health. Analyses were performed using STATA software version 13.1.
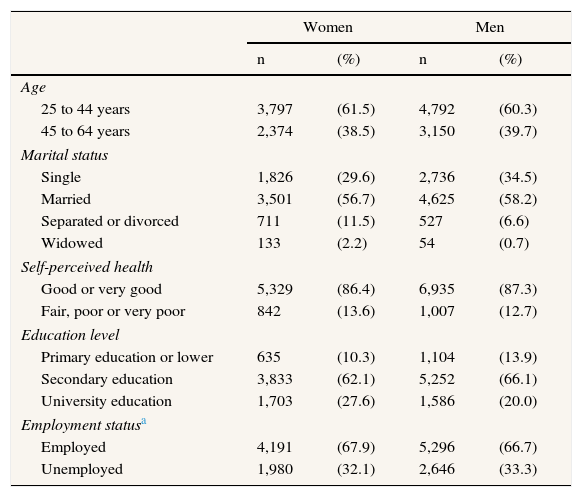
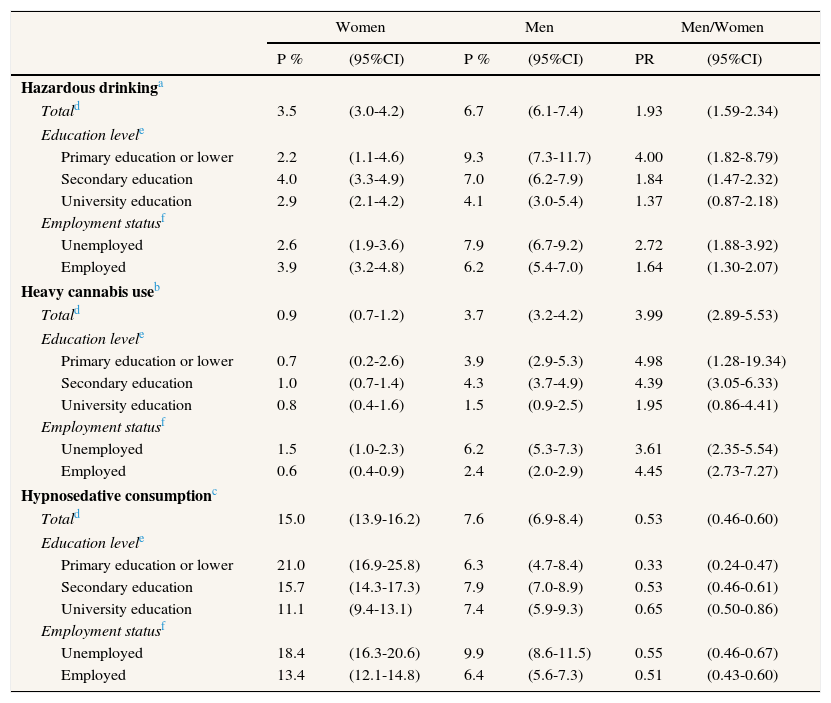
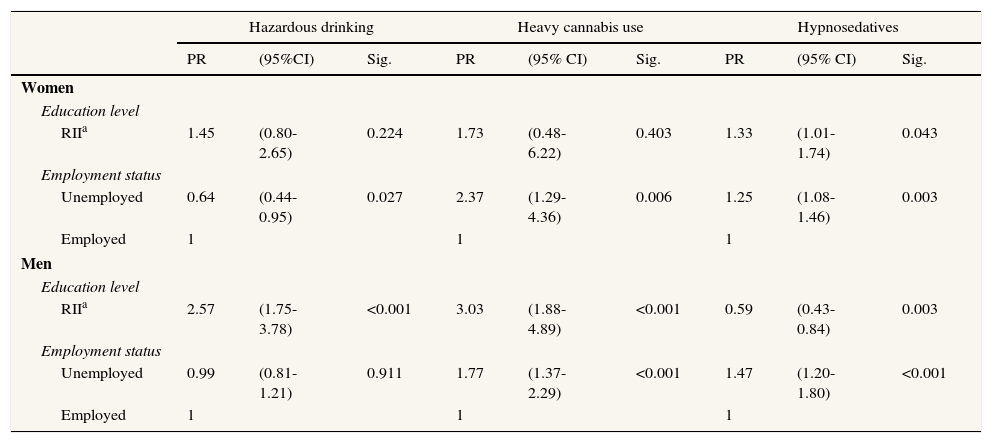
ResultsThe characteristics of the sample are shown in Table 1. The prevalence of hazardous drinking was higher in men (6.7%; 95%CI: 6.1-7.4) than in women (3.5%; 95%CI: 3.0-4.2). These sex differences were larger in people with only primary education, where the PR of hazardous drinking men/women was 4.00 (95%CI: 1.82-8.79) (Table 2). This was mainly due to the higher prevalence of hazardous drinking observed in men with lower education levels (RII=2.57; 95%CI: 1.75-3.78) while in women there was not a clear pattern (Table 3). In regards to the employment status, it was observed that differences were greater among unemployed people (the PR of hazardous drinking in unemployed men was 2.72 [95%CI: 1.88-3.92] times higher than in unemployed women), although these differences were not statistically significant (Table 2). In this case, this was mainly due to the lower prevalence of hazardous drinking in unemployed women compared to the employed women (RII=0.64; 95%CI: 0.44-0.95) (Table 3).
Distribution of age, marital status, self-perceived health, education level, employment status, hazardous drinking, heavy cannabis use and hipnosedative consumption separately for women and men. Spanish economically-active people aged 25-64 years. EDADES 2013.
| Women | Men | |||
|---|---|---|---|---|
| n | (%) | n | (%) | |
| Age | ||||
| 25 to 44 years | 3,797 | (61.5) | 4,792 | (60.3) |
| 45 to 64 years | 2,374 | (38.5) | 3,150 | (39.7) |
| Marital status | ||||
| Single | 1,826 | (29.6) | 2,736 | (34.5) |
| Married | 3,501 | (56.7) | 4,625 | (58.2) |
| Separated or divorced | 711 | (11.5) | 527 | (6.6) |
| Widowed | 133 | (2.2) | 54 | (0.7) |
| Self-perceived health | ||||
| Good or very good | 5,329 | (86.4) | 6,935 | (87.3) |
| Fair, poor or very poor | 842 | (13.6) | 1,007 | (12.7) |
| Education level | ||||
| Primary education or lower | 635 | (10.3) | 1,104 | (13.9) |
| Secondary education | 3,833 | (62.1) | 5,252 | (66.1) |
| University education | 1,703 | (27.6) | 1,586 | (20.0) |
| Employment statusa | ||||
| Employed | 4,191 | (67.9) | 5,296 | (66.7) |
| Unemployed | 1,980 | (32.1) | 2,646 | (33.3) |
Prevalence of hazardous drinking, heavy cannabis use and hypnosedative consumption by education level and employment status separately for women and men, and its association with sex through prevalence ratios and 95% confidence intervals. EDADES 2013.
| Women | Men | Men/Women | ||||
|---|---|---|---|---|---|---|
| P % | (95%CI) | P % | (95%CI) | PR | (95%CI) | |
| Hazardous drinkinga | ||||||
| Totald | 3.5 | (3.0-4.2) | 6.7 | (6.1-7.4) | 1.93 | (1.59-2.34) |
| Education levele | ||||||
| Primary education or lower | 2.2 | (1.1-4.6) | 9.3 | (7.3-11.7) | 4.00 | (1.82-8.79) |
| Secondary education | 4.0 | (3.3-4.9) | 7.0 | (6.2-7.9) | 1.84 | (1.47-2.32) |
| University education | 2.9 | (2.1-4.2) | 4.1 | (3.0-5.4) | 1.37 | (0.87-2.18) |
| Employment statusf | ||||||
| Unemployed | 2.6 | (1.9-3.6) | 7.9 | (6.7-9.2) | 2.72 | (1.88-3.92) |
| Employed | 3.9 | (3.2-4.8) | 6.2 | (5.4-7.0) | 1.64 | (1.30-2.07) |
| Heavy cannabis useb | ||||||
| Totald | 0.9 | (0.7-1.2) | 3.7 | (3.2-4.2) | 3.99 | (2.89-5.53) |
| Education levele | ||||||
| Primary education or lower | 0.7 | (0.2-2.6) | 3.9 | (2.9-5.3) | 4.98 | (1.28-19.34) |
| Secondary education | 1.0 | (0.7-1.4) | 4.3 | (3.7-4.9) | 4.39 | (3.05-6.33) |
| University education | 0.8 | (0.4-1.6) | 1.5 | (0.9-2.5) | 1.95 | (0.86-4.41) |
| Employment statusf | ||||||
| Unemployed | 1.5 | (1.0-2.3) | 6.2 | (5.3-7.3) | 3.61 | (2.35-5.54) |
| Employed | 0.6 | (0.4-0.9) | 2.4 | (2.0-2.9) | 4.45 | (2.73-7.27) |
| Hypnosedative consumptionc | ||||||
| Totald | 15.0 | (13.9-16.2) | 7.6 | (6.9-8.4) | 0.53 | (0.46-0.60) |
| Education levele | ||||||
| Primary education or lower | 21.0 | (16.9-25.8) | 6.3 | (4.7-8.4) | 0.33 | (0.24-0.47) |
| Secondary education | 15.7 | (14.3-17.3) | 7.9 | (7.0-8.9) | 0.53 | (0.46-0.61) |
| University education | 11.1 | (9.4-13.1) | 7.4 | (5.9-9.3) | 0.65 | (0.50-0.86) |
| Employment statusf | ||||||
| Unemployed | 18.4 | (16.3-20.6) | 9.9 | (8.6-11.5) | 0.55 | (0.46-0.67) |
| Employed | 13.4 | (12.1-14.8) | 6.4 | (5.6-7.3) | 0.51 | (0.43-0.60) |
EDADES: Spanish Household Survey on Alcohol and Drugs; 95%CI: 95% confidence interval; P: prevalence; PR: prevalence ratio.
In women hazardous drinking was considered when the total AUDIT score was 6 or more, while in men it was considered when the total AUDIT score was 8 or more.
Consumption of any hyposedative, including both prescription or non-prescription. The reference period for the three substances was the previous 12 months.
Prevalence ratios of hazardous drinking, heavy cannabis use and hypnosedative consumption by educational level and employment status and its 95% confidence intervals for women and men using Poisson regression models. EDADES 2013.
| Hazardous drinking | Heavy cannabis use | Hypnosedatives | |||||||
|---|---|---|---|---|---|---|---|---|---|
| PR | (95%CI) | Sig. | PR | (95% CI) | Sig. | PR | (95% CI) | Sig. | |
| Women | |||||||||
| Education level | |||||||||
| RIIa | 1.45 | (0.80-2.65) | 0.224 | 1.73 | (0.48-6.22) | 0.403 | 1.33 | (1.01-1.74) | 0.043 |
| Employment status | |||||||||
| Unemployed | 0.64 | (0.44-0.95) | 0.027 | 2.37 | (1.29-4.36) | 0.006 | 1.25 | (1.08-1.46) | 0.003 |
| Employed | 1 | 1 | 1 | ||||||
| Men | |||||||||
| Education level | |||||||||
| RIIa | 2.57 | (1.75-3.78) | <0.001 | 3.03 | (1.88-4.89) | <0.001 | 0.59 | (0.43-0.84) | 0.003 |
| Employment status | |||||||||
| Unemployed | 0.99 | (0.81-1.21) | 0.911 | 1.77 | (1.37-2.29) | <0.001 | 1.47 | (1.20-1.80) | <0.001 |
| Employed | 1 | 1 | 1 | ||||||
EDADES: Spanish Household Survey on Alcohol and Drugs; 95%CI: 95% confidence interval; RII: Relative Index of Inequalities; PR: prevalence ratio.
a Based on educational level.
For the three substances studied and for both sexes, the interaction between educational level and employment status was not statistically significant. For this reason, Table 3 only shows the models with the conjoint effect of these two independent variables and not the models that include its interaction. All models are adjusted for age, marital status, Spanish region of residence and self-perceived health. The reference period for the three substances was the previous 12 months.
The same results were observed for cannabis use. Men had higher prevalence of heavy cannabis use than women [3.7 (95%CI: 3.2-4.2) and 0.9 (95%CI: 0.7-1.2), respectively] and in lower levels of studies the sex differences were higher [PR men/women=4.98 (95%CI: 1.28-19.34)] (Table 2). This was because men with lower education levels were more heavy cannabis users than men with higher education (RII=3.03; 95%CI: 1.88-4.89), whereas in women there was not a clear pattern, just as in hazardous drinking (Table 3). Unlike what happens in hazardous drinking, the PR of heavy cannabis use in men/women was significantly higher among the employed (PR=4.45; 95%CI: 2.73-7.27) than among the unemployed (PR=3.61; 95%CI: 2.35-5.54), without statistically significant differences (Table 2). In Table 3, we observe significant differences in cannabis consumption according to the employment status, being the unemployed women and men more heavy cannabis users compared to the employed [RII=2.37 (95%CI: 1.29-4.36) and RII=1.77 (95%CI: 1.37-2.29), respectively].
Finally, in relation to hypnosedative use, the prevalence of consumption was higher in women than in men. 15.0% (95%CI: 13.9-16.2) of women had taken hypnosedatives in the last 12 months versus the 7.6% (95%CI: 6.9.-8.4) of men. In this case, the largest sex differences were also found among people with primary education or lower because women with lower education levels reported more consumption [21.0% (95%CI: 16.9-25.8) in women with primary education versus 11.1% (95%CI: 9.4-13.1) in women with higher education]. In men, there was no differences in hypnosedative consumption between the different levels of education (Table 2). Concerning hypnosedative consumption according to education level and employment status, statistically significant differences were found in both women and men, being women with lower educational level, men with university education and the unemployed in both sexes those with higher consumption (Table 3).
DiscussionIn our study, we found that among the Spanish economically-active population aged 25-64 the prevalence of hazardous drinking and heavy cannabis use was higher in men than in women, whereas the use of hypnosedatives was higher in women. The differences between men and women in substance use were higher in the lower educational levels. Regarding the influence of educational level on the use of the studied substances, in economically-active men, hazardous drinking and heavy cannabis use were negatively associated with education level, while hypnosedative use was positively associated. In economically-active women, only hypnosedative use was negatively associated with education level. Taking into account the employment status, being unemployed was related with higher heavy cannabis use and hypnosedative consumption, in both women and men and with lower hazardous drinking only in women, regardless of the educational level.
The main limitation of the study is its cross-sectional nature, which makes it necessary to consider a possible reverse causality, since we only have data about the consumption of the three substances in the last 12 months; in addition, there is no information on unemployment length nor on substance use history before losing their job.13 Using self-reported data might have led to a classification bias due to social desirability25 However, this could be mitigated by the anonymity of the surveys, the use of a separate self-completed questionnaire for the questions about substance use and the use of two validated tests (AUDIT19,20 and CAST21). Besides, the proportion of missing data about substance use is only around 3%. The use of educational level to estimate the SEP also deserves consideration. Since educational level is a multidimensional variable, the use of a more robust indicator than the education level would have been more appropriate. Still, it has been found that the level of studies is a good indicator of SEP in cross-sectional studies23. Another limitation is that we have not considered the influence of the alcohol industry's advertising on hazardous drinking and its possible different effect according to gender, educational level or employment status. However, it appears that gender differences in hazardous drinking are not explained by differences in alcohol advertising.26
The higher prevalence of hazardous drinking found in economically-active men in comparation to women is consistent with previous studies2,3,5 and could be due to biological and cultural reasons.1,2,17 Furthermore, the distribution of hazardous drinking by educational level suggests that alcohol consumption, as happened with tobacco, may has spread in the population according to the diffusion of innovations theory.27 From this perspective, alcohol consumption may have started, just as tobacco, becoming more generalised in men with higher educational level, extending later to men with lower educational level and to women.
Higher prevalence of hazardous drinking in economically-active men with lower educational level was found. This result could be explained by a greater tendency among men with this educational level to use alcohol to cope with stress.15 Besides, a low educational level may involve low-complexity jobs with fewer opportunities for stimulation or less social value. This type of work would not permit the access to certain benefits, such as income or prestige, so that the probability of drinking in response to stress would be higher.28 On the other hand, our results indicate, as other studies, a stronger association between unemployment and alcohol drinking in women than in men,17 being the prevalence of hazardous drinking in unemployed economically-active women lower than the employed economically-active women. As suggested by the literature,28,29 this could be explained by the possibility that the increasing occupation of positions with greater responsibility by women in the labour market may involve work situations related to alcohol consumption.
In economically-active women, the prevalence of heavy cannabis use is much lower than in economically-active men. As it has been suggested elsewhere,30 it is possible that for women the use of an illegal substance does not just mean engaging in a maladaptive behaviour, but may also be contrary to the social definition of how a woman should behave. In men, other studies point to an increased heavy cannabis use among those of lower educational level, which is confirmed by our study.12,31 Besides, a higher prevalence of heavy cannabis use among unemployed compared to the employed was found in both economically-active women and men, as also the literature suggests.13 Regarding the latter, unemployment has been described as one of the most important economic stressors.15 Thus, a higher heavy cannabis use could reflect a coping mechanism to deal with the economic stress due to the unemployment. When employment status is considered together with educational level, a higher prevalence of heavy use is observed among unemployed economically-active men and those with lower educational level. The traditional role of men as main breadwinners32 could explain this fact. Traditionally, men have had the main responsibility for productive work outside the home, while women were in charge of the care of people.1 Thereby men with lower educational level could be more likely to use substance to cope with the economic stress because of the unemployment, as they could have more economic difficulties than men with a higher educational level. However, we cannot rule out the possibility to lose a job as a result of a higher cannabis use. Besides, a previous study hypothesized that cannabis use during the adolescence may affect the future educational level and employment status.16
Unlike alcohol and cannabis, the prevalence of hypnosedative consumption was found to be higher in economically-active women than men. This greater consumption in women could be explained by a higher prevalence of mood disorders, depression and anxiety than men, as shown elsewhere.33 In fact, the ESEMeD-Spain study on mental disorders found a higher prevalence of this type of disorders among women34 and a consumption of psychoactive drugs that was almost three times higher among people with some mental disorder.7 In this sense, the way women handle and express anxiety and stress, and their greater propensity to seek medical care, would facilitate the diagnosis and treatment of mental disorders.8 Even if the factors that determine the treatment elections by health professionals are complex,7 it is possible that physicians have a greater tendency to prescribe psychoactive drugs for women than men35 regardless of their mental health status. On the other hand, the use of psychotropic medications in women could also be explained by the fact that they perceive them as less harmful,31 or because of a greater tendency to self-medicate.36 In relation to the educational level, economically-active women and men showed an opposite pattern: while in women were those with lower educational level the ones with higher hipnosedative consumption, in men the higher consumption was observed among those with higher educational level. In this sense, some studies suggest that the use of hypnosedatives as self-medication is more common among people with higher educational level.36 This higher prevalence may be due to greater knowledge of medications, more financial resources or a greater sense of personal autonomy, responsibility or control over their own health. As in other studies,4 we observed higher consumption of hypnosedatives in unemployed people inside the labour market regardless the educational level. This could be explained by a higher prevalence of mood and anxiety disorders in this group.34 This is relevant in a context of economic crisis, when the prevalence of poor mental health seems to increase, especially in unemployed men.18
ConclusionsThe study shows that there are differences between men and women in hazardous drinking, heavy cannabis use and hypnosedative consumption among economically-active people. While in women only a statistically significant pattern according to educational level is found in hypnosedatives consumption, in men higher educational level is associated with lower consumption of alcohol and cannabis and higher consumption of hypnosedatives. In relation to employment status, the unemployed women and men are those with higher cannabis and hypnosedative consumption, whereas the unemployed women are those with less alcohol consumption.
Unemployment during an economic crisis could increase mental health problems and substance use. However, little is known about differences between men and women in substance use in relation with educational level and employment status during the Spanish economic crisis.
What does this study add to the literature?There are differences between economically-active men and women in substance use. These differences are related with the educational level, being larger in the lowest educational level. Unemployed economically-active men and women had higher prevalence of substance use without differences between them. Specific preventive measures should consider gender equity to address men and women differently according to their level of education and employment.
María Teresa Ruiz Cantero.
Transparency declarationThe corresponding author on behalf of the other authors guarantee the accuracy, transparency and honesty of the data and information contained in the study, that no relevant information has been omitted and that all discrepancies between authors have been adequately resolved and described.
Authorship contributionsA. Espelt, M.J. Bravo and M. Bosque-Prous were involved in the conception and design of the study. E. Teixidó-Compañó and A. Espelt carried out the analysis and interpretation of data. The first version of the manuscript was written by E. Teixidó-Compañó and thereafter was improved by all authors, with important contributions. All authors have participated in writing the article, critical review and have approved the final version and are jointly responsible for adequate revision and discussion of all aspects included in the manuscript.
FundingThis research was supported by the Health Strategic Action grant (grant number PI13/00183), Spanish Network on Addictive Disorders (grant numbers RD12/0028/0018 and RD16/0017/0013), and had also the financial support of the Master of Public Health from the Universitat Pompeu Fabra, Barcelona, Spain. The 2013 Spanish Household Survey on Alcohol and Drugs (EDADES) was funded by the Government Delegation for the National Plan on Drugs. Ministry of Health and Social Policy.
Conflicts of interestNone.
The authors thank Giselle O’Connor for her review of English. This paper is part of the doctoral dissertation of Ester Teixidó-Compañó, at the Universitat Pompeu Fabra, Barcelona, Spain.









