



To estimate the percentage of adherence to highly-active antiretroviral therapy (HAART) in Spanish observational studies and to identify the variables associated with adherence.
MethodsSeven electronic databases were used to locate the studies. Six inclusion criteria were established. Two coders codified the variables independently. Intercoder reliability was calculated. Publication bias was analyzed through the Begg, Egger and Trim and Fill tests. Homogeneity was evaluated using the Q test and the l2 index. A random effects model was assumed to estimate both the overall percentage of adherence and to explain heterogeneity.
ResultsThis meta-analysis included 23 observational studies, yielding a total of 34 adherence estimates. The sample was composed of 9,931 HIV-positive individuals (72% men) older than 18 years under treatment with HAART. The percentage of patients adhering to an intake of >90% of the prescribed antiretroviral drugs was 55%. Wide heterogeneity was detected (I2=91.20; 95%CI: 88.75-93.13). Adherence was mainly measured using a single strategy (47.8%), the most widely used being self-report (48.7%). In the univariate analysis, the following factors were significant: infection stages A (β=0.68, p <0.001) and B (β=–0.56, p <0.01), viral loads >200 copies/ml (β=–0.41, p <0.05) and <200 (β=0.39, p <0.05), and university education (β=–0.66, p<0.05).
ConclusionsThe overall percentage of adherence was 55%, although this value may be an overestimate. Adherence was associated with infection stage A and with a viral load of <200 copies/ml.
Calcular el porcentaje de adherencia al TARGA en estudios observacionales españoles, así como identificar las variables asociadas a ella.
MétodosPara localizar los estudios se emplearon siete bases bibliográficas. Se establecieron seis criterios de inclusión. Dos codificadores realizaron la codificación de forma independiente. Se calculó la fiabilidad intercodificadores. El sesgo de publicación se evaluó mediante los tests de Begg y de Egger, y Trim & Fill. La homogeneidad se estimó mediante la prueba Q y el índice I2. Se asumió un modelo de efectos aleatorios tanto para la estimación del porcentaje global de adherencia como para explicar la heterogeneidad.
ResultadosEl metaanálisis incluyó 23 estudios observacionales que proporcionaron 34 estimaciones de la adherencia. La muestra está constituida por 9931 individuos VIH+ (72,2% hombres), mayores de 18 años y en tratamiento con TARGA. El porcentaje de pacientes con una adherencia al tratamiento de >90% de ingestión de los antirretrovirales prescritos fue del 55%. Se detectó una gran heterogeneidad (I2=91.20; IC95%: 88.75-93.13). La adherencia fue evaluada principalmente con una única estrategia (47,8%); el autoinforme fue la más empleada (48,7%). En el análisis univariado resultaron significativo los estadios A (β=0,68, p <0,001) y B (β=-0,56, p <0,01), la carga viral >200 copias/ml (β=-0,41, p <0,05) y <200 copias/ml (β=0,39, p <0,05), y el nivel de educación de estudios superiores (β=-0,66, p <0,05).
ConclusionesEl porcentaje global de adherencia fue del 55%, pero este valor puede estar sobrestimado. La adherencia se asoció al estadio A de la infección y a una carga viral <200 copias/ml.
Highly active antiretroviral therapy (HAART) has improved the clinical status and prognosis of most patients infected with HIV, decreasing their morbidity and mortality1–3. Therefore, since 1997 and coinciding with the widespread use of HAART, opportunistic infections have markedly decreased and the quality of life of HIV-infected patients has improved4.
Studies of the first HAART claimed that almost perfect adherence, classically greater than 95%5,6, was required to obtain maximal effectiveness. Recent studies have suggested that therapeutic objectives can be attained at lower levels of compliance in regimens based on non-nucleoside analog reverse-transcriptase and protease inhibitors boosted with ritonavir, especially in patients who achieved undetectable viremias7–10.
Although viral suppression is feasible with moderate levels of adherence to HAART, several studies have shown that the emergence of resistant strains11,12 and mortality13 increase with lower adherence.
Although many studies have evaluated adherence to HAART and its associated variables, their results vary depending on how adherence was measured, the characteristics of the samples, and the remaining variables analyzed. A systematic review identifying and explaining these discrepancies is required to increase adherence to HAART.
In Spain, the prevalence of HIV is around three infections per thousand inhabitants14. Although the incidence of AIDS has markedly decreased since the new antiretroviral treatments began to be used, Spain remains one of the countries with the highest incidence of AIDS in Western Europe15,16. In this country, antiretroviral medicines are administered free of charge through the medical pharmacological services of the public health system. The overall annual expenditure on these medicines has been estimated to be more than a seventh of the total medical pharmacological expenditure17,18.
No meta-analyses of adherence to HAART in the Spanish population have been published. The number of studies on adherence to HAART in Spain has increased, allowing them to be systematically reviewed and to shed light on the design and improvement of studies of HAART adherence interventions.
The objective of this study was to carry out a meta-analysis of HAART adherence in Spain and to synthesize observational studies in order to estimate average adherence and identify the variables associated with this adherence.
MethodsSearch strategy and study selectionThe studies were selected from (a) seven electronic databases (PsycInfo, Medline, IME, EMI, Teseo, IBECS, ISOC and ISI Web of Knowledge) using a boolean search on the title of any type of publication: {[HAART OR highly active antiretroviral therapy] AND adheren* AND [HIV OR AIDS OR (human immu* virus) OR (acquired immu* syndrome)] AND [Spanish OR Spain]}; (b) Web browsers; (c) the summary of the latest conference proceedings; (d) funded projects on HIV / AIDS in Spain and (e) tracing of references cited in others studies. The studies had to be written either in English or in Spanish.
Studies were included in the review if they (a) aimed to evaluate adherence to HAART in a Spanish sample, (b) had a cross-sectional or cohort design, (c) evaluated an HIV-positive sample over 18 years old under treatment with HAART, (d) measured adherence at least once and using one strategy, (e) established an intake of >90% or 95% of the medication prescribed as the cut-off point for adherence, and (f) provided sufficient information to obtain the proportion of adherence to HAART.
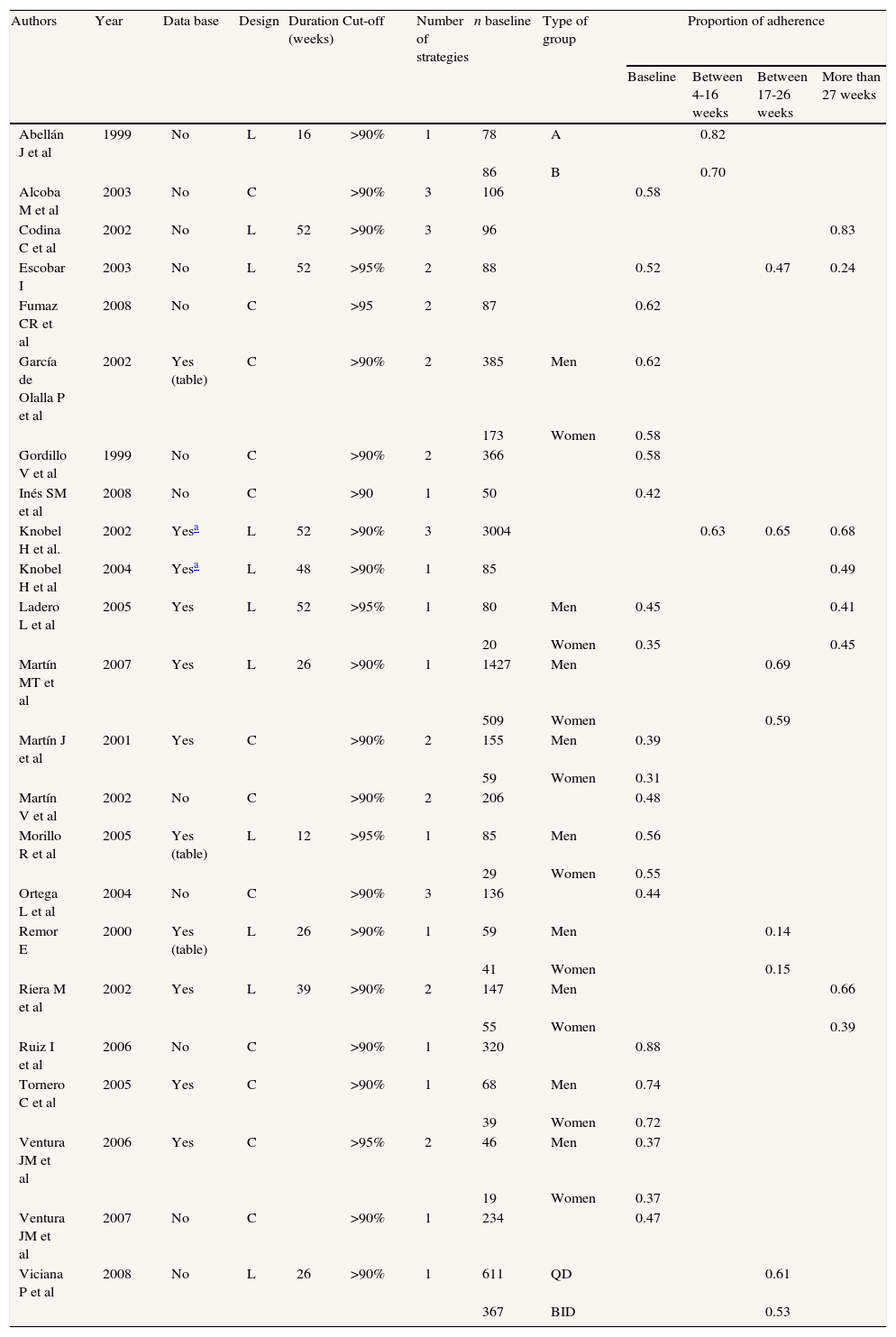
The search ended on September 13, 2009 and studies from 1998 were included. Twenty-three independent studies that met the six selection criteria were included in this meta-analysis (table 1). These 23 primary studies19–41 provided 34 estimates of adherence to HAART. In three studies20,32,34 the total independence among their samples could not be checked.
Description of the studies included in the meta-analysis.
| Authors | Year | Data base | Design | Duration (weeks) | Cut-off | Number of strategies | n baseline | Type of group | Proportion of adherence | |||
| Baseline | Between 4-16 weeks | Between 17-26 weeks | More than 27 weeks | |||||||||
| Abellán J et al | 1999 | No | L | 16 | >90% | 1 | 78 | A | 0.82 | |||
| 86 | B | 0.70 | ||||||||||
| Alcoba M et al | 2003 | No | C | >90% | 3 | 106 | 0.58 | |||||
| Codina C et al | 2002 | No | L | 52 | >90% | 3 | 96 | 0.83 | ||||
| Escobar I | 2003 | No | L | 52 | >95% | 2 | 88 | 0.52 | 0.47 | 0.24 | ||
| Fumaz CR et al | 2008 | No | C | >95 | 2 | 87 | 0.62 | |||||
| García de Olalla P et al | 2002 | Yes (table) | C | >90% | 2 | 385 | Men | 0.62 | ||||
| 173 | Women | 0.58 | ||||||||||
| Gordillo V et al | 1999 | No | C | >90% | 2 | 366 | 0.58 | |||||
| Inés SM et al | 2008 | No | C | >90 | 1 | 50 | 0.42 | |||||
| Knobel H et al. | 2002 | Yesa | L | 52 | >90% | 3 | 3004 | 0.63 | 0.65 | 0.68 | ||
| Knobel H et al | 2004 | Yesa | L | 48 | >90% | 1 | 85 | 0.49 | ||||
| Ladero L et al | 2005 | Yes | L | 52 | >95% | 1 | 80 | Men | 0.45 | 0.41 | ||
| 20 | Women | 0.35 | 0.45 | |||||||||
| Martín MT et al | 2007 | Yes | L | 26 | >90% | 1 | 1427 | Men | 0.69 | |||
| 509 | Women | 0.59 | ||||||||||
| Martín J et al | 2001 | Yes | C | >90% | 2 | 155 | Men | 0.39 | ||||
| 59 | Women | 0.31 | ||||||||||
| Martín V et al | 2002 | No | C | >90% | 2 | 206 | 0.48 | |||||
| Morillo R et al | 2005 | Yes (table) | L | 12 | >95% | 1 | 85 | Men | 0.56 | |||
| 29 | Women | 0.55 | ||||||||||
| Ortega L et al | 2004 | No | C | >90% | 3 | 136 | 0.44 | |||||
| Remor E | 2000 | Yes (table) | L | 26 | >90% | 1 | 59 | Men | 0.14 | |||
| 41 | Women | 0.15 | ||||||||||
| Riera M et al | 2002 | Yes | L | 39 | >90% | 2 | 147 | Men | 0.66 | |||
| 55 | Women | 0.39 | ||||||||||
| Ruiz I et al | 2006 | No | C | >90% | 1 | 320 | 0.88 | |||||
| Tornero C et al | 2005 | Yes | C | >90% | 1 | 68 | Men | 0.74 | ||||
| 39 | Women | 0.72 | ||||||||||
| Ventura JM et al | 2006 | Yes | C | >95% | 2 | 46 | Men | 0.37 | ||||
| 19 | Women | 0.37 | ||||||||||
| Ventura JM et al | 2007 | No | C | >90% | 1 | 234 | 0.47 | |||||
| Viciana P et al | 2008 | No | L | 26 | >90% | 1 | 611 | QD | 0.61 | |||
| 367 | BID | 0.53 | ||||||||||
C: cross-sectional; L: longitudinal; A: conventional medical assessment; B: protocolized assessment; QD: once-daily dosing; BID: twice-daily dosing.
The authors of 21 of the 23 primary studies included in the meta-analysis were emailed to request information on the databases they had used in their studies or at least a set of data that would allow two groups to be constructed: men and women. Nineteen authors responded to the message. The databases of eight studies and additional data from three studies were received.
CodingTwo independent trained raters coded each study following the coding manual (available from the main author on request). The final coding form registered 42 variables, which were grouped into three sets: “extrinsic”, of the “design” and the “sample”.
Although no scale to assess the methodological quality was used, a small group of variables related to the methodological design were coded to compare adherence according to the studies’ characteristics.
Calculation of effect sizes and study outcomesThe proportion of adherence to HAART was estimated in each study as the effect size index. When, due to gender or location, more than one group could be drawn from a study, separate estimates of adherence were calculated for each group. If adherence was measured with more than one strategy, the average adherence was calculated. If the study evaluated adherence at different time points, the first assessment of adherence was chosen to avoid dependence, although a sensitivity analysis was performed for each set of measurements including all the possible comparisons. Because the length of follow-up varied widely across studies, we divided outcomes into four measurement intervals as a strategy to examine all study assessments: between 0-3 weeks (k=21), between 4-16 weeks (k=3), between 17-26 weeks (k=6), more than 27 weeks (k=4).
To ensure the normality of the effect size index, all the statistics were obtained using a logit transformation of the proportion of adherence (T=lnp1−p), where p was the proportion of adherence for each comparison. Then, the meta-analysis using a random effect model weighted by the inverse variance was performed. Finally, all the results were transformed back to a proportion for a more comprehensive interpretation of the data using the formula42p=eT1+eT. This outcome ranges from 0 to 1, where 1 indicates that all the patients have achieved high adherence (at least >90%), while 0 indicates that no patient has exceeded this cut-off point.
Homogeneity was evaluated using the Q test and the I2 index with its confidence interval43. The relationship among study dimensions and the proportion of adherence variability was examined by using modified least squares regression analyses with weights equivalent to the inverse of the variance for each effect size. When feasible factors related significantly to the proportion of adherence, they were entered into a series of models controlling for intercorrelations among the maintained study dimensions. These combined models allowed determination of the extent to which variation might be exclusively attributed to surviving study dimensions or not. The continuous variables that were significant in the univariate analyses were zero-centered to reduce multicollinearity44; if they were categorical, dummy variables were created44. Models with simultaneous independent variables were created if these factors were registered in more than five studies (k >5) and under mixed-effects assumptions, which are considered to have more conservative statistical power45.
The publication bias was analyzed through three different strategies: Trim and Fill46, Begg's strategy47, and the Egger test48.
ResultsStudy and adherence characteristics, and sampleThe characteristics of the 23 primary studies were as follows: 21 (91.3%) studies were published and two (8.7%) were unpublished (doctoral theses), 10 (43.5%) were written in English and 13 (56.5%) in Spanish, 12 (52.2%) had a cross-sectional design and 11 (47.8%) a longitudinal design. All of the studies were performed between 1998 and 2008.
Patients with an intake of >90% of prescribed HAART were considered adherent. Adherence was assessed using just one strategy in 11 studies (47.8%), two strategies in eight (34.8%) and three strategies in four (17.4%). Self-report was the most frequently used strategy to quantify adherence in 19 studies (48.7%), followed by registration of dispensing medicines in 11 (28.2%), plasma drug concentration in four (10.3%), counting of surplus medication in two (5.1%), viral load in two (5.1%) and electronic devices in one (2.6%).
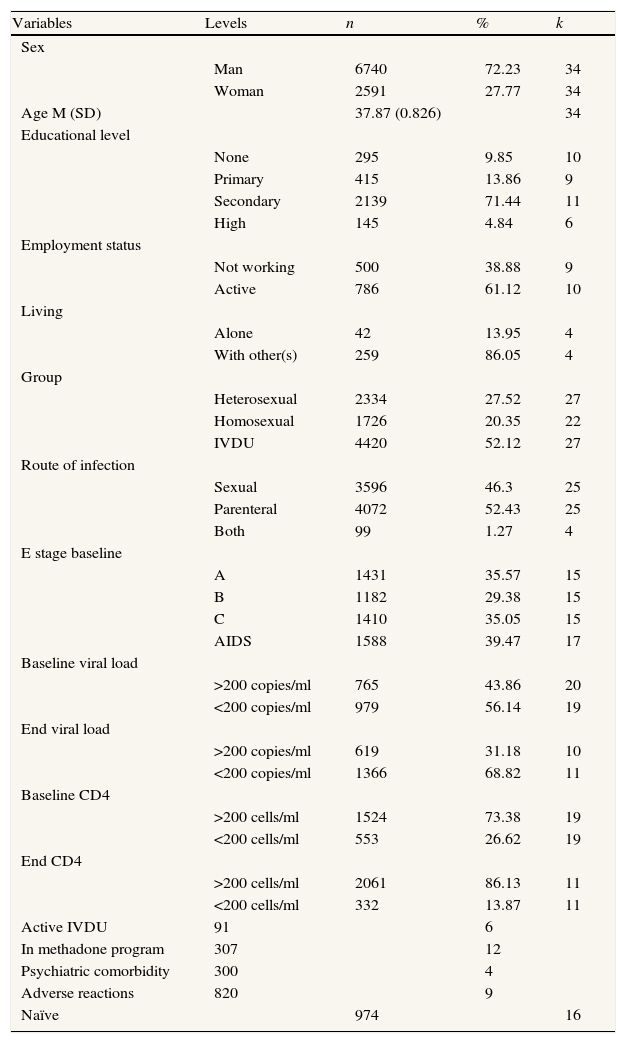
From the 23 studies included in table 1, a sample (table 2) composed of 9,331 HIV-positive patients older than 18 years under HAART was obtained, with 6,740 (72.2%) men and 2,591 (27.8%) women and a mean age of 37.9 years (SD: 2.83, range: 33-44).
Description of the sample.
| Variables | Levels | n | % | k |
| Sex | ||||
| Man | 6740 | 72.23 | 34 | |
| Woman | 2591 | 27.77 | 34 | |
| Age M (SD) | 37.87 (0.826) | 34 | ||
| Educational level | ||||
| None | 295 | 9.85 | 10 | |
| Primary | 415 | 13.86 | 9 | |
| Secondary | 2139 | 71.44 | 11 | |
| High | 145 | 4.84 | 6 | |
| Employment status | ||||
| Not working | 500 | 38.88 | 9 | |
| Active | 786 | 61.12 | 10 | |
| Living | ||||
| Alone | 42 | 13.95 | 4 | |
| With other(s) | 259 | 86.05 | 4 | |
| Group | ||||
| Heterosexual | 2334 | 27.52 | 27 | |
| Homosexual | 1726 | 20.35 | 22 | |
| IVDU | 4420 | 52.12 | 27 | |
| Route of infection | ||||
| Sexual | 3596 | 46.3 | 25 | |
| Parenteral | 4072 | 52.43 | 25 | |
| Both | 99 | 1.27 | 4 | |
| E stage baseline | ||||
| A | 1431 | 35.57 | 15 | |
| B | 1182 | 29.38 | 15 | |
| C | 1410 | 35.05 | 15 | |
| AIDS | 1588 | 39.47 | 17 | |
| Baseline viral load | ||||
| >200 copies/ml | 765 | 43.86 | 20 | |
| <200 copies/ml | 979 | 56.14 | 19 | |
| End viral load | ||||
| >200 copies/ml | 619 | 31.18 | 10 | |
| <200 copies/ml | 1366 | 68.82 | 11 | |
| Baseline CD4 | ||||
| >200 cells/ml | 1524 | 73.38 | 19 | |
| <200 cells/ml | 553 | 26.62 | 19 | |
| End CD4 | ||||
| >200 cells/ml | 2061 | 86.13 | 11 | |
| <200 cells/ml | 332 | 13.87 | 11 | |
| Active IVDU | 91 | 6 | ||
| In methadone program | 307 | 12 | ||
| Psychiatric comorbidity | 300 | 4 | ||
| Adverse reactions | 820 | 9 | ||
| Naïve | 974 | 16 |
n: number of subjects; k: number of studies; %: percentage of individuals; IVDU: intravenous drug user.
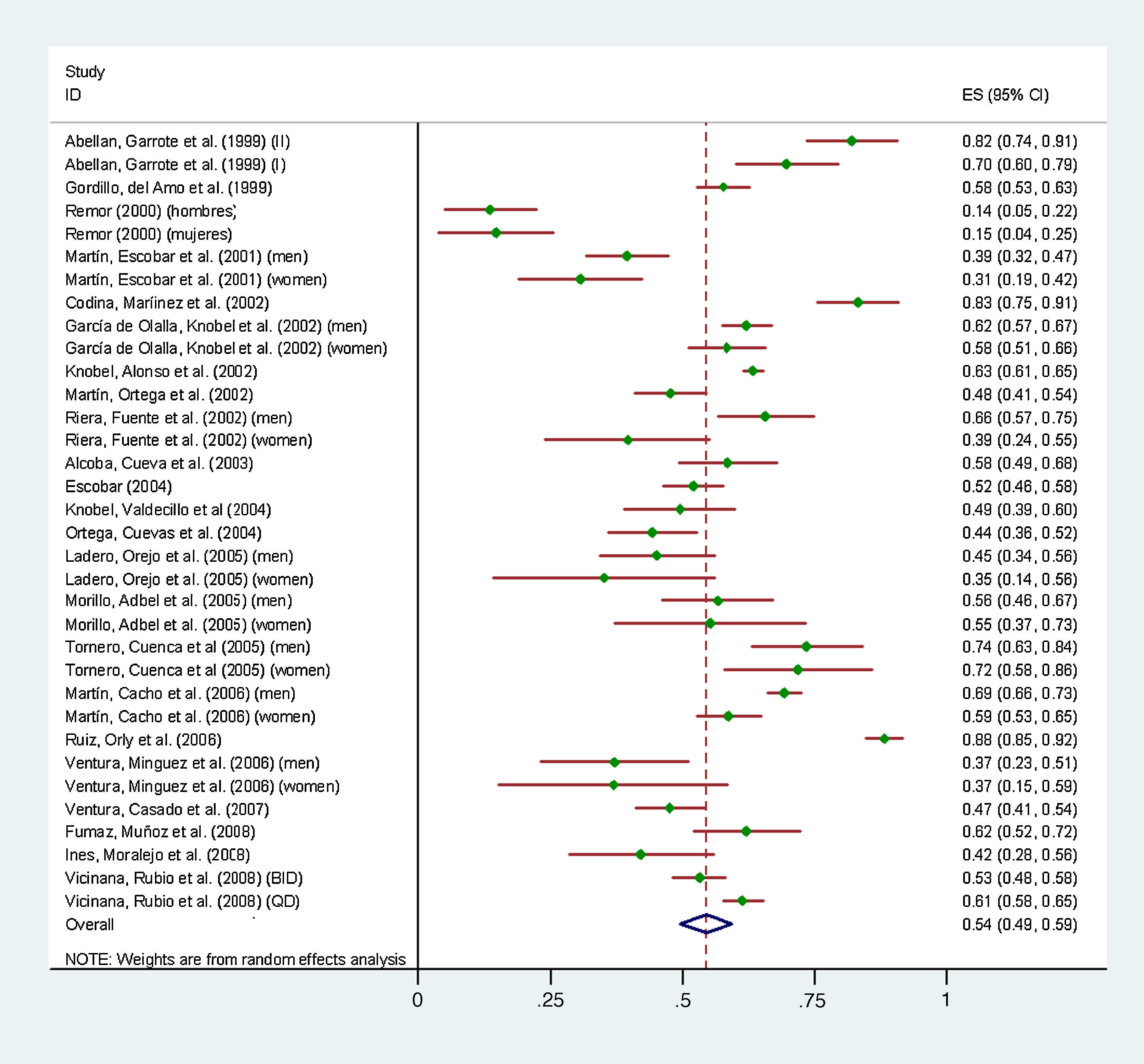
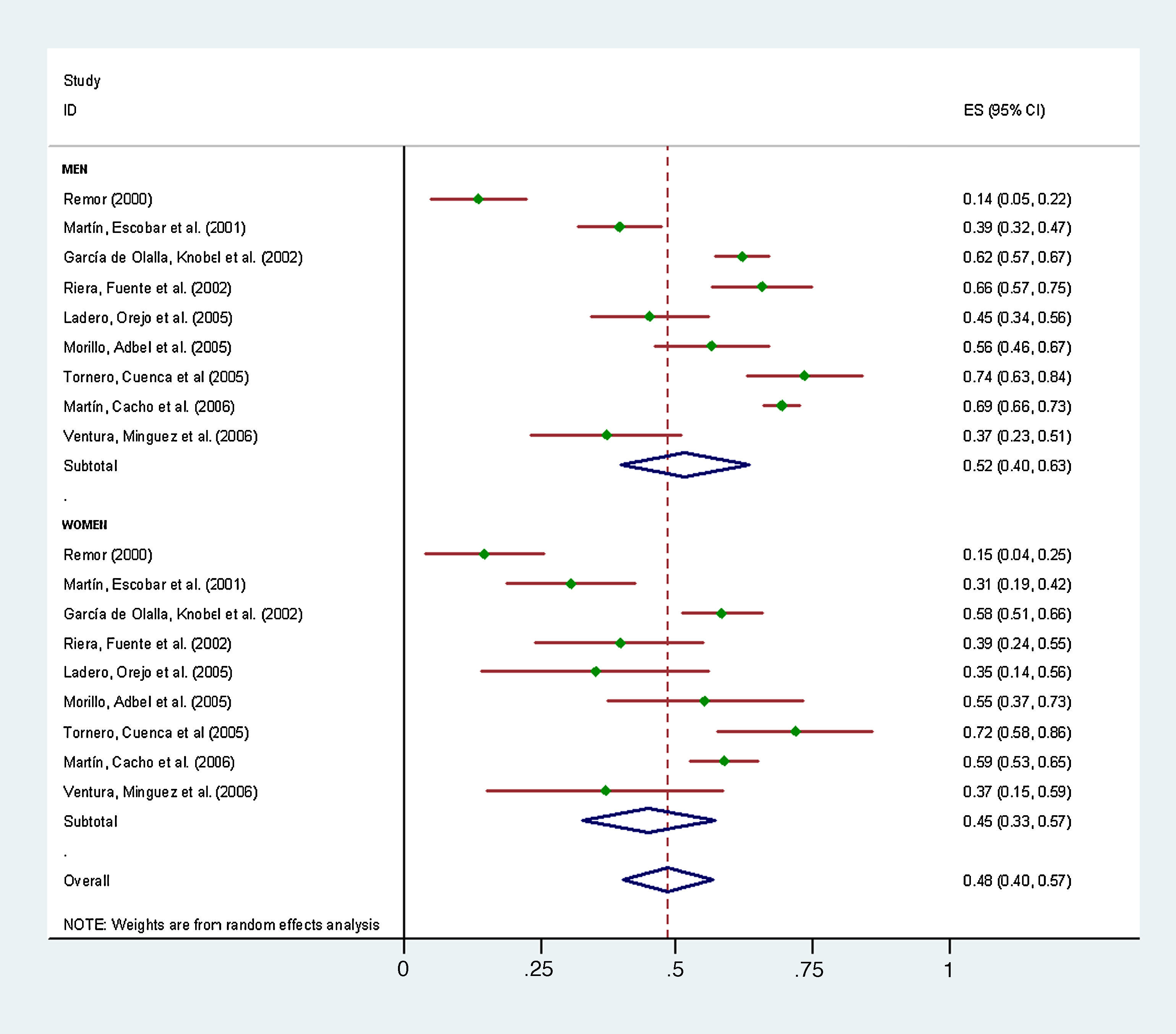
The average adherence to HAART under the random effects model for the Spanish sample was 0.54 (95%CI: 0.49-0.59), showing wide heterogeneity (I2=91.20; 95%CI: 88.75-93.13) under the fixed-effects model. Therefore, only the results under the random-effects model and mixed-effects model to explain the heterogeneity not explained by the model (I2=51%; 95%CI: 11.45-72.88) are presented. Chart 1 shows the forest plot of the proportion of adherence of the 34 groups as well as the overall mean proportion of adherence (at the bottom of the chart). Chart 2 shows the proportion of adherence by sex.


A sensitivity analysis was performed to (i) test the influence of possible outliers, (ii) test the patterns of the set of studies divided by the week of measurement, and (iii) determine whether the results were affected by the exclusion of some studies in which the total independence among their samples could not be checked. Comparison of all the possible outliers revealed that none worked as a real outlier. The time interval showed the same patterns when the data were analyzed by interval as a separate meta-analysis rather than as a moderator without inclusion of more than one measurement per study. Finally, we decided to maintain all studies with a likely dependence because their exclusion did not affect the final results but would involve a substantial loss of information.
Intercoder reliability was higher than 0.90. Cohen's kappa was used for categorical variables (κ=0.98) and the Spearman-Brown correlation coefficient for continuous variables (r=0.955). Disagreements were solved through discussion.
The three tests used to assess possible publication bias aimed to show absence of bias. These tests were the Trim and Fill (the results indicate that there are no missing studies), Begg's test (z=–0.10, p=0.922) and Egger's test (bias=-1.58, t=–1.98, p=0.054).
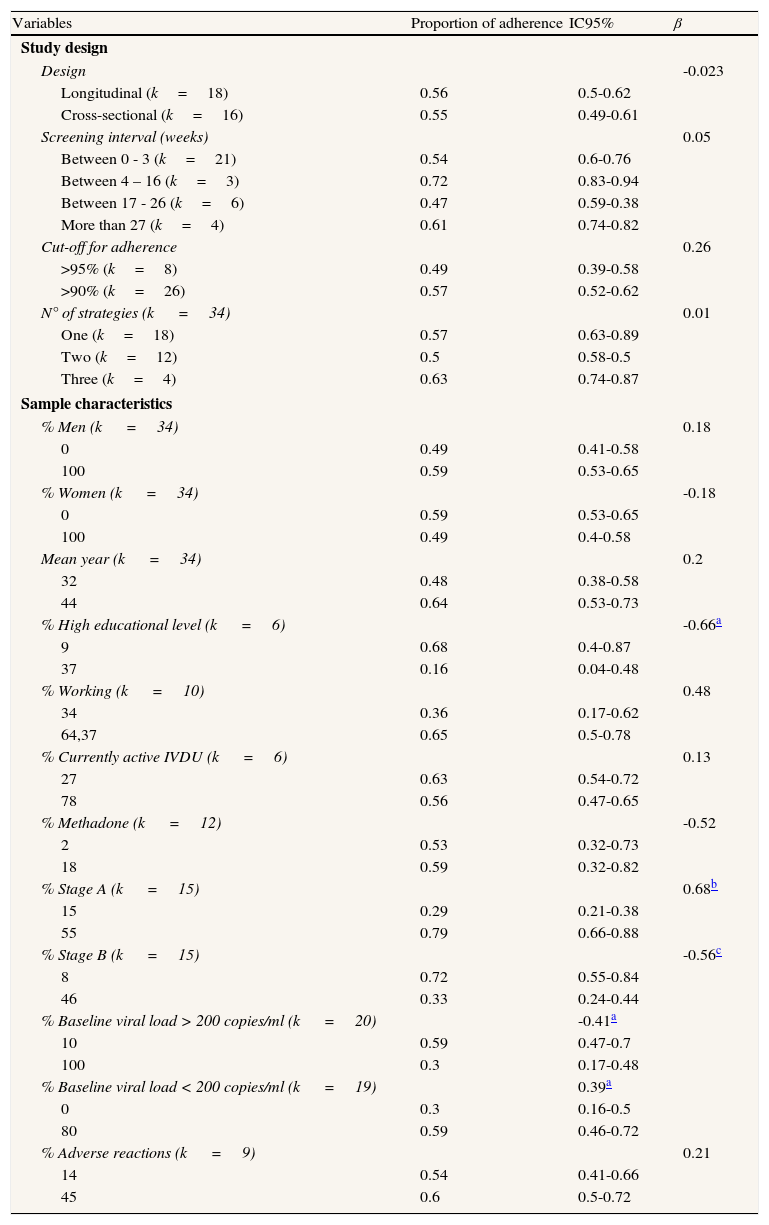
Factors modifying adherence to HAARTA higher percentage of participants in stage A and with baseline viral load <200 copies/ml showed greater adherence. However, lower adherence was found when a higher percentage of patients were in stage B, with a baseline viral load >200 copies/ml, and with a high level of education, that is, education from secondary school onwards (table 3; this table depicts the variables registered in more than five groups, k >5).
Univariate analysis. Mixed effects model.
| Variables | Proportion of adherence | IC95% | β |
| Study design | |||
| Design | -0.023 | ||
| Longitudinal (k=18) | 0.56 | 0.5-0.62 | |
| Cross-sectional (k=16) | 0.55 | 0.49-0.61 | |
| Screening interval (weeks) | 0.05 | ||
| Between 0 - 3 (k=21) | 0.54 | 0.6-0.76 | |
| Between 4 – 16 (k=3) | 0.72 | 0.83-0.94 | |
| Between 17 - 26 (k=6) | 0.47 | 0.59-0.38 | |
| More than 27 (k=4) | 0.61 | 0.74-0.82 | |
| Cut-off for adherence | 0.26 | ||
| >95% (k=8) | 0.49 | 0.39-0.58 | |
| >90% (k=26) | 0.57 | 0.52-0.62 | |
| N° of strategies (k =34) | 0.01 | ||
| One (k=18) | 0.57 | 0.63-0.89 | |
| Two (k=12) | 0.5 | 0.58-0.5 | |
| Three (k=4) | 0.63 | 0.74-0.87 | |
| Sample characteristics | |||
| % Men (k =34) | 0.18 | ||
| 0 | 0.49 | 0.41-0.58 | |
| 100 | 0.59 | 0.53-0.65 | |
| % Women (k =34) | -0.18 | ||
| 0 | 0.59 | 0.53-0.65 | |
| 100 | 0.49 | 0.4-0.58 | |
| Mean year (k =34) | 0.2 | ||
| 32 | 0.48 | 0.38-0.58 | |
| 44 | 0.64 | 0.53-0.73 | |
| % High educational level (k =6) | -0.66a | ||
| 9 | 0.68 | 0.4-0.87 | |
| 37 | 0.16 | 0.04-0.48 | |
| % Working (k =10) | 0.48 | ||
| 34 | 0.36 | 0.17-0.62 | |
| 64,37 | 0.65 | 0.5-0.78 | |
| % Currently active IVDU (k =6) | 0.13 | ||
| 27 | 0.63 | 0.54-0.72 | |
| 78 | 0.56 | 0.47-0.65 | |
| % Methadone (k =12) | -0.52 | ||
| 2 | 0.53 | 0.32-0.73 | |
| 18 | 0.59 | 0.32-0.82 | |
| % Stage A (k =15) | 0.68b | ||
| 15 | 0.29 | 0.21-0.38 | |
| 55 | 0.79 | 0.66-0.88 | |
| % Stage B (k =15) | -0.56c | ||
| 8 | 0.72 | 0.55-0.84 | |
| 46 | 0.33 | 0.24-0.44 | |
| % Baseline viral load > 200 copies/ml (k =20) | -0.41a | ||
| 10 | 0.59 | 0.47-0.7 | |
| 100 | 0.3 | 0.17-0.48 | |
| % Baseline viral load < 200 copies/ml (k =19) | 0.39a | ||
| 0 | 0.3 | 0.16-0.5 | |
| 80 | 0.59 | 0.46-0.72 | |
| % Adverse reactions (k =9) | 0.21 | ||
| 14 | 0.54 | 0.41-0.66 | |
| 45 | 0.6 | 0.5-0.72 | |
IVDU=intravenous drug user.
Some of the significant moderators showed high collinearity (rs > 0.90, e.g., stage A and stage B, the two variables for baseline viral load) and therefore separate combined models were tested by different groups of moderators, avoiding dependence among them and excluding high educational level due to the small number of studies reporting this data (k=6). After all the possible combinations of stage and baseline viral load, the only variable that remained significant when baseline viral load (> 200 copies/ml because this value was measured in the largest number of studies) was controlled for was the percentage of patients in stage A. The model explaining 52% of the variance, more than expected by chance, was stage A (β=0.69, p=0.0005) controlling by baseline viral load > 200 copies /ml (β=–0.21, p=0.30), yielding the following regression equation (expressed in the unstandardized coefficients, the B values): –1.637+0.060 x (stage A) –0.0078 (baseline viral load > 200 copies/ml).
DiscussionThe main result of this study is that adherence to HAART in Spain is 55%. This percentage is similar or slightly lower than that found by other authors in individuals from different populations worldwide49–55. However, in this meta-analysis, this value could be overestimated for two reasons: firstly, adherence was assessed by a single strategy in more than half of the primary studies and secondly, because the most widely used strategy was self-report.
When the variable of baseline viral load < 200 copies/ml was controlled for, the higher the percentage of patients in stage A, the greater the adherence. Other studies have also found lower adherence in patients with high viral loads than in those with low loads56,57. The stage of infection was closely related to the viral load, indicating the importance of controlling for this variable in the final model. In this meta-analysis, the higher percentage of subjects in stage A, the greater the adherence, whereas the higher percentage of subjects in stage B, the lower the adherence. Similarly, several authors found greater adherence in patients with a shorter time since infection58–60. Quality of life61, degree of distress62 and patients’ expectations of treatment could be determining variables in these results.
Although the level of education was significant, this variable was only registered in six studies. Thus, more research is needed to enable generalizations related to this moderator to be made.
This meta-analysis also codified other variables that several studies have found to be associated with higher adherence: male gender63–67, older age68–72, having a stable job58,59,73, not having adverse reactions50,63,66,73–76, not consuming illegal drugs53,65,66,76–79, not drinking alcohol53,65,74,79, not having psychiatric comorbidity49,50,53,77,78,80 and having some support49,58,78. Although all these variables were significant in the univariate level and under a fixed effects model, they lost their significance in order to assume a random effects model.
One of the limitations of this study is the small number of variables registered in the primary studies. Spanish studies assessing adherence to HAART are generally highly restrictive in the number of variables analyzed, often limited to recording the most common demographic, biological or pharmacological variables, without recording those that seem to play a role of equal or greater weight in the adherence to HAART, such as psychosocial variables. Although this meta-analysis codified 42 variables, most could not be used in the multivariate analysis given the small percentage of studies that recorded them, which significantly restricted the analysis of heterogeneity.
Another limitation is the wide heterogeneity of this meta-analysis. The small number of studies identified to form part of this meta-analysis also played a decisive role in these limitations.
Adherence to the HAART in Spanish samples should continue to be assessed in order to determine variability and improve adherence. However, adherence should be measured by more than one strategy to avoid its overestimation and follow experts recommendations81. Assessments of adherence should record a larger number of variables because, although many of the variables codified in this meta-analysis were significant, the small number of studies that recorded them prevented this model from being employed as an explanatory model. Finally, stage A and viral baseline load < 200 copies/ml were significantly associated with higher adherence, whereas stage B and viral baseline load > 200 copies/ml were associated with lower adherence. Therefore, programs aimed at maintaining and increasing adherence should be aware of both patients’ stage of infection and their viral baseline load.
Adherence to HAART should be approached from multidisciplinary, multifactorial and biopsychosocial per spectives. Greater collaboration among researchers would help to gain further knowledge and reduce duplication of efforts82.
Author contributionsC. Ortego and T.B. Huedo-Medina conceptualized the study, analyzed the data, and led the writing of the manuscript. J. Vejo assisted with the acquisition and content coding. F.J. LLorca assisted with the conceptualization of the study and the data interpretations. Every author provided valuable critical revisions of the manuscript and also agreed in both contents and form of the final version, being C. Ortego the responsible of this article.
Funding/supportProject financed by IFIMAV. N/Ref.: PSG 10/02
Conflicts of interestThe authors indicate no conflicts of interest.
We thank study authors who made their data available for this study. Juan Botella who assisted in advising statistically and revising the coding manual, Julia del Amo for their assessment in the search of epidemiological information, and Soledad Fernandez for reviewing the English translation.











