



To explore the decisional process of people living with human immunodeficiency virus (HIV) currently enrolled in antiretroviral clinical trials.
MethodCross-sectional retrospective study. Outcome variables were reasons to participate, perceived decisional role (Control Preference Scale), the Decisional Conflict Scale and the Decisional Regret Scale. Descriptive statistics were calculated, and associations among these variables and with sociodemographic and clinical characteristics were analyzed with non-parametric techniques.
ResultsMain reasons to participate were gratitude towards Fundación Huesped (47%), the doctor's recommendation (32%), and perceived difficulty to access treatment in a public hospital (28%). Most patients thought that they made their decision alone (54.8%) or collaboratively with the physician (43%). Decisional conflict was low, with only some conflict in the support subscale (median=16.67). Education was the only significant correlate of the total decisional conflict score (higher in less educated patients; p=0.018), whereas education, recent diagnosis, living alone, lower age, being man and doctor's recommendation to go to Fundación Huésped related to higher conflict in different subscales. Nobody regretted to participate.
ConclusionsThe decision making regarding participation in HIV trials, from the perspective of participants, was made respecting their autonomy and with very low decisional conflict. Currently, patients show no signs of regret. However, even in this favorable context, results highlight the necessity of enhancing the decision support in more vulnerable patients (e.g., less educated, recently diagnosed or with less social support), thus warranting equity in the quality of the decision making process.
Explorar el proceso de decisión de las personas que viven con el virus de la inmunodeficiencia humana (VIH) y participan en ensayos clínicos de antirretrovirales.
MétodoEstudio retrospectivo transversal. Las variables de resultado fueron los motivos para participar, el rol de participación percibido (Escala de preferencia de control), la Escala de conflicto decisional y la Escala de arrepentimiento decisional. Se realizó una estadística descriptiva y se establecieron asociaciones entre estas variables con variables sociodemográficas y clínicas usando técnicas no paramétricas.
ResultadosLas razones para participar fueron la gratitud hacia la Fundación Huésped (47%), la recomendación del médico (32%) y la dificultad percibida para acceder al tratamiento en un hospital público (28%). Los pacientes opinan que tomaron su decisión solos (54,8%) o en colaboración con el médico (43%). El conflicto en la decisión fue bajo, aunque hubo cierto conflicto en la subescala de apoyo (mediana=16,67). La educación se relacionó con el conflicto en la decisión (mayor en pacientes con menor nivel educativo; p=0.018), mientras que la educación, el diagnóstico reciente, vivir solo, la menor edad y la recomendación del médico de ir a la Fundación Huésped se relacionaron con un mayor conflicto en diferentes subescalas. Nadie se arrepintió de su participación.
ConclusionesDesde la perspectiva de los participantes, en el proceso de toma de decisiones se respetó su autonomía, hubo poco conflicto decisional y no aparecen signos de arrepentimiento. A pesar de este contexto favorable, los resultados destacan la necesidad de mejorar el apoyo a las decisiones en las personas más vulnerables (con menos educación, de diagnóstico reciente o con menos apoyo social) para garantizar la equidad en la calidad del proceso de decisión.
Clinical trials are essential to assessing new therapies and advancing evidence-based treatments. Currently, the vast majority of research about factors that influence participation in clinical trials, as well as interventions to improve it, has been carried out in the field of cancer,1,2 in which only a small percentage of patients consent to participate.3 Results have shown that barriers to participate exist at different levels, related to the patient, the trial, or contextual factors. Among personal factors, cultural and linguistic diversity, lower income, or less trust in the physician or the health system are associated to a lower participation.4 Regarding the trial, uncertainties related to randomization and the benefit/risk balance of the intervention investigated are basic aspects in the decision to participate.5 Finally, contextual factors such as distance to the research centre, the number of required visits or medical tests also play an important role in potential participants’ decision.3
The few existing studies with patients diagnosed with human immunodeficiency virus (HIV) considering participation in clinical trials have focused on issues associated with the informed consent process,6 ethnic minorities recruitment,7,8 or on barriers and motivators to participate in vaccination of people at high risk of infection.9,10 A recent systematic review of qualitative studies in sub-Saharan Africa (including studies of vaccination or treatment) concluded that participation in HIV research is associated with considerable fear and uncertainty.11 Both feelings are influenced by social relationships, socioeconomic and domestic factors, the research clinic context and the relationships with research staff. Although these studies have produced a valuable knowledge about the psychological experience of HIV patients considering trial participation, specific variables related to the decision-making process (e.g., preference and perception of involvement, decisional conflict and regret) remain mostly unexplored. In standard care settings, research on HIV patients’ participation is also very scarce; the few existing studies show that a majority of patients want to be involved in the decision about treatment,12–14 and that this preference is associated to a better adherence to antiretroviral treatment.12 Patients presented more decisional conflict (i.e., uncertainty about treatment uptake) when they did not perceive this desired level of participation.13
This study aims to explore the decisional process of people with HIV currently enrolled in clinical trials about pharmacological treatment. Specifically, we want to describe: 1) patients’ motives for participating in the clinical trial; 2) their perceived decisional role; 3) the level of decisional conflict; 4) their current regret about trial participation; and 5) associations among these variables as well as with sociodemographic and clinical factors.
MethodThis cross-sectional retrospective study was conducted from November 2016 to February 2017 in the Fundación Huésped, a not-for-profit organization located in Buenos Aires (Argentina), that offers health and education services to people at risk or diagnosed with transmissible diseases, especially HIV.
SampleFundación Huésped is one of the main clinical research sites for HIV in Argentina, having participated in several national and international multisite clinical trials of antiretroviral treatment. This treatment is not included in the usual services provided by the institution (since it is covered by the national health system), and only patients participating in clinical trials have access to it in Fundación Huésped. Inclusion criteria were adult diagnosed with HIV, participating in a HIV trial at Fundación Huésped, and having signed the informed consent for trial participation within the previous year. During the recruitment period, approximately 150 patients were participating in several clinical trials. Doctors at Fundación Huésped explained the study and invited to consecutive eligible patients, and those who agreed signed consent and were individually interviewed by a researcher. The study was approved by the Research Ethics Committee of the Fundación Huésped (Study Fh-23).
Measures- •
Sociodemographic: age, sex, education, income (whether it covers basic needs or not), job status, living alone (yes/no), country of origin.
- •
Clinical: time since diagnosis (more/less than 1 year), disease transmission (dichotomized into “Man who has sex with man vs. other”), and viral load (detectable/undetectable).
- •
Decision-making:
- -
Control variables: months after signing informed consent, previous participation in clinical trials (yes/no), whether they actively asked for participation in the trial (yes/no), time to make the decision (the same day/later).
- -
Reasons to participate: conjointly with doctors at Fundación Huésped who recruit participants for clinical trials, we developed a list of reasons/facilitators to participate in the trial (yes/no format): 1) patient did not know where to go; 2) not having employment-based (private) health insurance (due to being unemployed); 3) perceived difficult to access treatment in a public hospital (due to bureaucracy, waiting lists); 4) their doctor recommended to go to Fundación Huésped; 5) feeling well treated or in debt with Fundación Huésped; 6) preferring a modern treatment; 7) doing good to other patients; 8) pressure to participate by the family; and 9) pressure to participate by their doctor.
- -
Perceived decisional role was assessed with one item from the Control Preference Scale,15 but with three response options instead of five (mainly or only them/shared decision/the practitioner).
- -
Decisional conflict was assessed retrospectively with the Spanish version of the Decisional Conflict Scale (DCS).16 It has 16 items and five subscales: informed (about the alternatives, benefits and risks of the clinical trial), values (feeling clear about personal values associated with the potential consequences of the clinical trial), support (having advice and no pressure in decision-making), uncertainty (being clear about the choice) and effectiveness (feeling that the decision was informed and congruent with own values). Patients were encouraged to respond how they felt when making the decision to participate in the trial. Scores were transformed to a 0-100 scale (higher scores indicates more conflict).
- -
Regret about trial participation was assessed with the Decision Regret Scale (DRS, 5 items from completely agree to completely disagree).17 The original English scale was translated into Spanish by the authors and then back-translated by an independent bilingual researcher. There were only a few discrepancies between the two versions, which were resolved by consensus.
- •
Subjective experience about trial participation: patients were asked if they had felt like a guinea pig (yes/no), and whether they had told their doctors about that (yes/no). They also were required to briefly explain, in an open answer, why they continued in the trial.
Descriptive statistics were calculated (means, medians, standard deviations, interquartile ranges, percentages). Associations between categorical variables were assessed by means of χ2 test. Due to the asymmetric distribution of the DCS total score and subscales, we used non-parametric tests for analyses. In order to check the validity of the retrospective measure of decisional conflict (total score), its associations with the four control variables were analyzed; we expect a null association with time since informed consent was signed (Spearman's correlation and Kruskal-Wallis’ test, categorizing time in 0-3, 4-6, 7-9, and 10-12 months), and lower conflict in patients with previous experience in clinical trials, in those who actively asked for participating, and in those who consented the same day they were invited (Mann-Whitney's U-test).
For the remaining independent variables (sociodemographic, clinical, decisional), Mann-Whitney's U-test was used to identify those related to the DCS (total score and subscales) and DRS. The perceived decisional role showed only two subjects who responded “mainly or only the practitioner”, and therefore only the two other categories were compared. Analyses were conducted with SPSS 21.0.
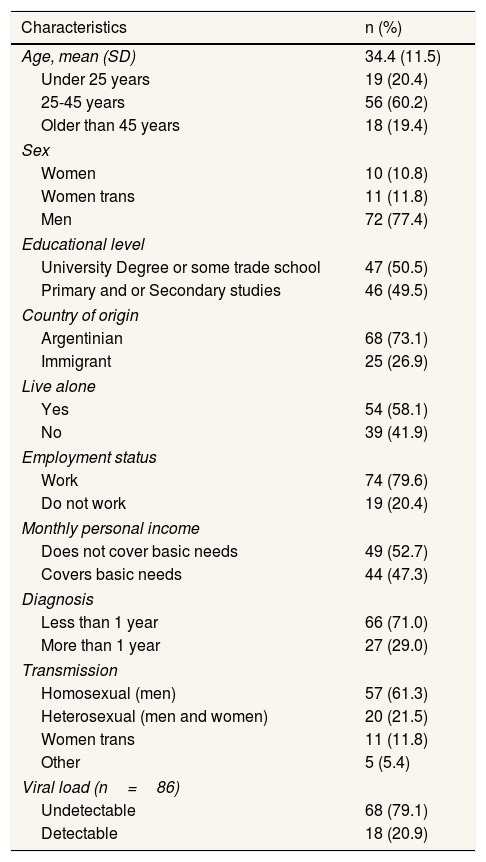
ResultsNinety-nine consecutive patients enrolled in clinical trials were invited to participate, and 93 agreed. Mean age was 34.4 and 77.4% were men. Approximately half of the sample had only primary or secondary studies, 58.1% lived alone and almost one-third were immigrants. Most worked (79.6%) but a 52.7% had a salary insufficient to cover basic needs. Seventy-one per cent had the HIV diagnosis within the previous year, and 88.2% were enrolled in their first clinical trial (Tables 1 and 2).
Sociodemographic and clinical characteristics of participants (N=93).
| Characteristics | n (%) |
|---|---|
| Age, mean (SD) | 34.4 (11.5) |
| Under 25 years | 19 (20.4) |
| 25-45 years | 56 (60.2) |
| Older than 45 years | 18 (19.4) |
| Sex | |
| Women | 10 (10.8) |
| Women trans | 11 (11.8) |
| Men | 72 (77.4) |
| Educational level | |
| University Degree or some trade school | 47 (50.5) |
| Primary and or Secondary studies | 46 (49.5) |
| Country of origin | |
| Argentinian | 68 (73.1) |
| Immigrant | 25 (26.9) |
| Live alone | |
| Yes | 54 (58.1) |
| No | 39 (41.9) |
| Employment status | |
| Work | 74 (79.6) |
| Do not work | 19 (20.4) |
| Monthly personal income | |
| Does not cover basic needs | 49 (52.7) |
| Covers basic needs | 44 (47.3) |
| Diagnosis | |
| Less than 1 year | 66 (71.0) |
| More than 1 year | 27 (29.0) |
| Transmission | |
| Homosexual (men) | 57 (61.3) |
| Heterosexual (men and women) | 20 (21.5) |
| Women trans | 11 (11.8) |
| Other | 5 (5.4) |
| Viral load (n=86) | |
| Undetectable | 68 (79.1) |
| Detectable | 18 (20.9) |
SD: standard deviation.
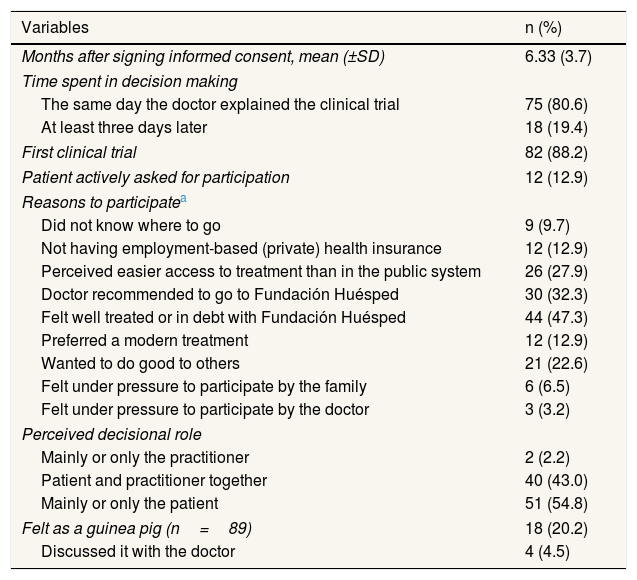
Variables related to the decisional process regarding participation in HIV clinical trials (N=93).
| Variables | n (%) |
|---|---|
| Months after signing informed consent, mean (±SD) | 6.33 (3.7) |
| Time spent in decision making | |
| The same day the doctor explained the clinical trial | 75 (80.6) |
| At least three days later | 18 (19.4) |
| First clinical trial | 82 (88.2) |
| Patient actively asked for participation | 12 (12.9) |
| Reasons to participatea | |
| Did not know where to go | 9 (9.7) |
| Not having employment-based (private) health insurance | 12 (12.9) |
| Perceived easier access to treatment than in the public system | 26 (27.9) |
| Doctor recommended to go to Fundación Huésped | 30 (32.3) |
| Felt well treated or in debt with Fundación Huésped | 44 (47.3) |
| Preferred a modern treatment | 12 (12.9) |
| Wanted to do good to others | 21 (22.6) |
| Felt under pressure to participate by the family | 6 (6.5) |
| Felt under pressure to participate by the doctor | 3 (3.2) |
| Perceived decisional role | |
| Mainly or only the practitioner | 2 (2.2) |
| Patient and practitioner together | 40 (43.0) |
| Mainly or only the patient | 51 (54.8) |
| Felt as a guinea pig (n=89) | 18 (20.2) |
| Discussed it with the doctor | 4 (4.5) |
SD: standard deviation.
The most frequent reasons to participate in the trial were having feeling well treated or in debt with Fundación Huésped (47.3%), the doctor's recommendation of going there (32.3%), perceived difficulties to access treatment in the public system (27.9%), and the desire of doing good to other patients (22.6%) (Table 2). Only a 12.9% stated that they preferred a modern treatment, and very few felt pressured by their doctor (3.2%) or family (6.5%).
Gratitude towards Fundación Huésped significantly related to the perceived difficulty to access to treatment in a public hospital (χ2=12.7; p <0.001) and not having employment-based insurance (12.9%) (χ2=7.17; p=0.007).
Decisional roleMost patients thought that they made their decision alone (54.8%) or shared the decision with the doctor (43.3%) (Table 2). None of the sociodemographic, clinical and motives-related variables significantly differed between these two groups.
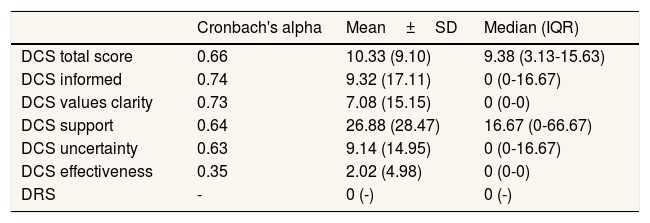
Decisional conflictCronbach's alpha for the DCS total score was 0.66 (Table 3). The subscales ranged 0.63-0.74, except effectiveness, which showed a value of 0.35. The Kolmogorov-Smirnov's test for normality yielded a p-value of 0.095 for the total score and p <0.001 for the subscales, with scores asymmetrically distributed towards low levels of conflict. The median total score was 9.38 (interquartile range [IQR]: 3.13–15.63), and four subscales obtained medians of zero. The subscale with higher median was support (16.67; IQR: 0–66.67).
Participants’ decisional conflict (retrospectively assessed) and regret with the decision (range: 0-100).
| Cronbach's alpha | Mean±SD | Median (IQR) | |
|---|---|---|---|
| DCS total score | 0.66 | 10.33 (9.10) | 9.38 (3.13-15.63) |
| DCS informed | 0.74 | 9.32 (17.11) | 0 (0-16.67) |
| DCS values clarity | 0.73 | 7.08 (15.15) | 0 (0-0) |
| DCS support | 0.64 | 26.88 (28.47) | 16.67 (0-66.67) |
| DCS uncertainty | 0.63 | 9.14 (14.95) | 0 (0-16.67) |
| DCS effectiveness | 0.35 | 2.02 (4.98) | 0 (0-0) |
| DRS | - | 0 (-) | 0 (-) |
DCS: Decisional Conflict Scale; DRS: Decisional Regret Scale; IQR: interquartile range; SD: standard deviation.
The DCS was not significantly related to the time elapsed since the informed consent for trial participation was signed (Spearman's r=0.08; p=0.461), nor after categorizing time into four periods (Kruskal-Wallis’ test; p=0.621). Compared to their counterparts, conflict was lower in patients who asked for participation (n=12; U=299; p=0.031). Results of having previous experience in clinical trials (n=11; U=297; p=0.066), and having signed informed consent the same day of the invitation (n=75; U=532, p=0.161) were in the expected direction of lower conflict, but they did not reach significance.
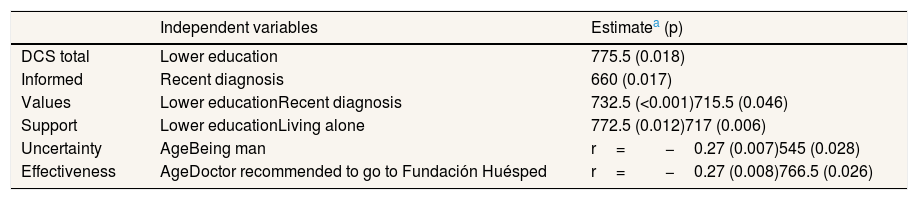
Table 4 shows the significant univariate correlates of the DCS. Lower education related to more conflict in the total score and the subscales values and support, whereas informed and uncertainty obtained p-values of 0.069 and 0.066, respectively (in the latter, however, the association was in the contrary direction). For informed and values, a recent diagnosis (<1 year) was significantly associated to more conflict. Living alone related to less perceived support. For uncertainty, significant correlates were being man and lower age. Finally, the perceived effectiveness of the decision was lower in younger patients and in those recommended to go to Fundación Huésped by their doctor (none of the remaining motives-related variables or the perceived decisional role significantly related to decisional conflict). We did not perform the planned multiple regression analyses for the subscales, because their non-normality did not resolve after several arithmetic transformations. Nonetheless, there were only two predictors in each model, and they were unrelated in all cases.
Univariate significant correlates of decisional conflict.
| Independent variables | Estimatea (p) | |
|---|---|---|
| DCS total | Lower education | 775.5 (0.018) |
| Informed | Recent diagnosis | 660 (0.017) |
| Values | Lower educationRecent diagnosis | 732.5 (<0.001)715.5 (0.046) |
| Support | Lower educationLiving alone | 772.5 (0.012)717 (0.006) |
| Uncertainty | AgeBeing man | r=−0.27 (0.007)545 (0.028) |
| Effectiveness | AgeDoctor recommended to go to Fundación Huésped | r=−0.27 (0.008)766.5 (0.026) |
DCS: Decisional Conflict Scale.
All participants scored zero on the DRS.
Subjective experienceThere was four missing responses to this question (n=89). Eighteen patients (20.2%) reported having felt like a guinea pig, and only four of them told about that with the doctor. Open answers revealed that in most cases that subjective feeling had not emotional negative consequences, and that participants understood that clinical trials are necessary to obtained health benefits for them or for other people with HIV.
DiscussionThis study explored retrospectively the decisional process of patients with HIV, enrolled in clinical trials evaluating antiretroviral treatments, as well as their current regret. Among the assessed reasons/facilitators for trial participation, those associated with the personal experience with Fundación Huésped (i.e, gratitude towards the institution due to the services it offers to patients, doctor's recommendation, and easy access to treatment through clinical trials) have been more frequent than a desire for modern treatments, altruistic motives or external pressures. The sample recruited had a considerable level of economic deprivation (52% stated having a monthly income which does not cover their basic needs), and although treatment for HIV is covered by the national health system, more than a quarter of participants perceived an easier access in Fundación Huésped (due to excessive bureaucracy and waiting lists in the public system).
These patients’ characteristics could make them more vulnerable to pressures to participate from doctors or their family, but results showed that very few participants perceived this pressure, and most thought that they had decided autonomously or in collaboration with the doctor. Professionals in Fundación Huésped have not specific formation in shared decision making, beyond their personal attitudes and abilities in the interaction with patients. In standard care settings, where shared decision-making is advocated as the gold standard in diagnostic or treatments decisions,18,19 a perception of being included in treatment decisions has been shown to be associated to less decisional conflict, in HIV13 and other conditions20,21 (we could not test this association since only two patients perceived not to be involved in the decision). In the scenario of clinical trials, however, there is usually more uncertainty about treatment's benefits and risks, and the concept of informed (vs. shared) decision-making could be seen more appropriate, due to ethical and legal concerns. However, many patients prefer and/or perceive a collaborative decision process with professionals,22 as it has occurred in our sample.
In the trade-off between motives/psychological needs favoring participation in the trial, and its perceived potential harms or inconveniences, the former clearly prevailed as reflected in the low level of decisional conflict reported. We cannot know the quality of participants’ objective knowledge about the trials’ benefits and risks when making the decision; previous research has shown that less objectively informed participants were more likely to participate.23 Patients in our sample stated being well informed about the potential benefits and harms of the clinical trial (subscale informed), clear about the importance they attribute to those consequences (values) and sure about the decision (uncertainty, effectiveness). The retrospective nature of the measure could influence these results, since the current satisfaction with participation in the trial (reflected in the complete absence of decisional regret) might introduce a positive retrospective bias. The validity tests performed were in the predicted direction (even in a context of a floor effect), but the risk is not disposable. The effectiveness subscale is possibly the most likely to be sensible to retrospective bias, since it can be seen as a reverse measure of regret, and in fact it obtained by far the lowest mean score.
The subscale support was the only one which showed some level of conflict. A majority of participants (58%) lived alone, and this variable significantly related to worse scores on this subscale. On the other hand, previous research has shown that disclosure of HIV status is an important stressor because it may expose people to stigma, discrimination, abandonment, violence and moral challenges.24 Most of our participants had been diagnosed within the previous year and enrolled in the trial a mean of 6.6 months ago. Therefore, it is likely that a number of them still had not shared with many people their fears and uncertainty associated with living with HIV and starting treatment, increasing their feeling of being unsupported.
A lower education level was the only significant predictor of the decisional conflict total score. This association is possibly mediated by a better understanding of doctor's explanations about the trial in more educated patients, since knowledge of the disease and the therapeutic procedures has been shown to be related to less decisional conflict in other medical conditions.25 Other psychological variables like decisional self-efficacy could also mediate this result.26,27 Therefore, a correct understanding of clinical trials’ procedures and outcomes in less educated patients must be enhanced, as occurs with other vulnerable populations such as rural28 or ethnic minorities.29 Educational and decision support interventions (e.g., decision aids) could help to fill these gaps in knowledge, promoting an actual informed decision and also improving attitudes towards clinical trials.30
Patients did not show decisional regret at all. Previous research about trial participation has focused mainly on the phase of invitation and acceptance, but few studies have analyzed participants’ regret.31–33 In standard care settings in other medical conditions, both the decisional conflict when making treatment decisions, and the subsequent occurrence of adverse effects, have been shown to be associated (among other factors) with later regret.34,35 Both variables could be responsible of the complete absence of decisional regret in our sample.
LimitationsThis study was a first approximation to the decisional process about participation in HIV trials, and it has several limitations. The sample was relatively small and represents only part of the “picture”, since it included mostly recently diagnosed patients who consented to participate in trials for initial HIV treatment, and among these, those who have not discontinued their participation due to adverse effects or other reasons. Furthermore, results are not generalizable to other socioeconomic contexts or health systems. Second, carrying out the study in the Fundación Huésped increases the risk of social desirability bias, possibly contributing to the low level of conflict and regret reported. Third, as discussed above, the assessment of decisional variables, except regret, was retrospective, which could be subjected to memory or reconstruction bias. Fourth, the floor effect observed in the DCS could obscure its associations with the remaining variables. Finally, we assessed multiple associations between many variables without adjusting the significance level, with the subsequent increase in the risk of type I error; however, the few significant associations found mostly have a clear theoretical sense.
ConclusionsDespite its limitations, this study contributes to the limited evidence on HIV patients’ decision-making regarding participation in clinical trials. In this sample of HIV patients, the decision-making in a clinical trial was perceived retrospectively as respectful with their autonomy and with a very low level of decisional conflict. Participation was mainly driven by a feeling of reciprocity towards a non-profit organization which offers support and education services for patients. Even in this favorable scenario, results highlight the necessity of enhancing the decision support in more vulnerable patients (e.g., less educated, recently diagnosed, or in those with less social support), thus warranting equity in the quality of the decision making process. More research is needed to determine predictors of participation in HIV trials and the quality of the decision process.
There are few studies with patients diagnosed with human immunodeficiency virus (HIV) focused on participation in clinical trials. The decision-making process of people living with HIV invited to participate in antiretroviral clinical trial remains mostly unexplored. Participation in HIV research is associated with considerable fear and uncertainty.
What does the study add to literature?Many participants thought they shared the decision to participate with their physicians even though in clinical trials is encouraged the informed decision-making. Decisional conflict was low and nobody regretted participation. Education significantly related to less conflict in the total score of the decisional conflict scale and the subscales values and support. Living alone significantly related to less perceived support in the decision. People newly HIV diagnosed, with low education or living alone, should be paid special attention in the informed consent process.
Azucena Santillán.
Transparency declarationThe corresponding author on behalf of the other authors guarantee the accuracy, transparency and honesty of the data and information contained in the study, that no relevant information has been omitted and that all discrepancies between authors have been adequately resolved and described.
Authorship contributionsAll authors made substantial contributions to conception and design of this study. Feijoo-Cid & Sued, worked in the design and conceptin of the work. Feijoo-Cid & Rivero-Santana performed data analysis. All authors contributed to the interpretation of data. Feijoo-Cid, Rivero-Santana & Sued were involved in drafting the manuscript and the rest of the authors revised it critically for important intellectual content. All authors gave final approval of the version to be published.
AcknowledgementsWe thank all participants who generously answered the questionnaire. We also thank Horacio Beylis, Emanuel Fojo, Virginia Salazar and Fernanda Nadir Cardozo for their contributions to the recruitment process, R Paul Kerston for the review and editing of the manuscript. David Moriña acknowledges financial support from the Spanish Ministry of Economy and Competitiveness, through the María de Maeztu Programme for Units of Excellence in R&D (MDM-2014-0445) and from Fundación Santander Universidades.
FundingThis research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflicts of interestThe authors declare that there is no conflict of interest.











