



The 3rd International Nursing and Health Sciences Students and Health Care Professionals Conference (INHSP)
Más datosThe study was aimed to determine the influence of the determinant of anemia in pregnancy in the district Polewali Mandar, Indonesia.
MethodsThis study uses a cross-sectional design analysis. The subject in this study was the third-trimester pregnant mother with a sample amount of 80 people selected using the cluster sampling technique.
ResultsThe majority of this study showed that as much as 93.8% of the third-trimester pregnant women were suffering from anemia, and 6.8% of the third-trimester pregnant women were not subjected to anemia. Based on statistical test results using the Chi-Square test obtained that age (P-value=0.644), education (P-value=0.003), economic Status (P-value=0.138), Antenatal care visit (P-value=0.584), nutritional Status (P-value=0.929), parity (P-value=0.380), Pregnancy distance (P-value=0.776), consumption of iron tablets (P-value=0.036) and worm infections (P-value=0.821). Results showed that two determinants significantly affect anemia in pregnancy, and seven determinants did not significantly affect anemia in pregnancy Regency of Polewali Mandar.
ConclusionA significantly related determinant in the study is the education and consumption of iron tablets.
Anemia in pregnancy is defined as a condition in which pregnant women have a hemoglobin level of less than 11.0g/dl in the first and third trimesters or hemoglobin levels less than 10.5g/dl in the II trimester. Anemia is a common blood disorder when the level of red blood cells (erythrocytes) in the body becomes too low or decreased.1,2
Anemia includes health problems with the highest prevalence in pregnant women. WHO reported that 52% of pregnant women have anemia in developing countries. Based on the results of Basic Health Research (Riskesdas) year 2013 in Indonesia, the prevalence of anemia in pregnant women is 37.1%, and in 2018 now the prevalence rate of anemia is 48.9%, it has increased from the year 2013.3,4
Anemia will cause conditions with a sense of fatigue, weakness, dizziness, and paleness. The impact of anemia in pregnancy that is not treated will cause abortus, premature uterine atony, and bleeding until shock. 1,5 Based on the Government Health Office of Polewali Mandar, the distribution of pregnant mothers in the year 2016 is 2546 (23.1%) cases of 9293 pregnant women. In 2017 pregnant women anemia 2605 (25.5%) cases of 9272 pregnant women while in the year 2018, the number of pregnant women anemia calculated from January to September, namely as much as 1,684 with the number of pregnant mothers 6070. Most of the incidence of anemia is found in health centers Pekkabata, Matakali, Katumbangan, and Campalagian. This study was aimed to explore the determinant of anemia in pregnancy in the district Polewali Mandar, Indonesia.
MethodThe type of research used was cross-sectional; it was conducted in the working area of Puskesmas Pekkabata, Matakali, Katumbangan, and Campalagian in Polewali Mandar district, South Sulawesi, Indonesia. Center of the area where the research is chosen because it is a place with the highest incidence of anemia each year compared with other health centers. This study was conducted for 3months. The samples used in this study were the third-trimester pregnant mothers.
The measurement of hemoglobin in the third trimester of pregnant women uses the Family Digital tool, designed explicitly for hemoglobin examination done by blood-impregnation at the end of the patient. Age data collection, economic status education, antenatal care visits, nutritional status, parity, and pregnancy distances are obtained from questionnaires and interviews. Consumption of iron tablets in the results of interviews and see the maternal and child health book. Nutritional Status Data is derived from the results of the upper arm circumference measurement. The Data of parasitic worm infection is obtained from solid stool test results in the Parasitology laboratory.
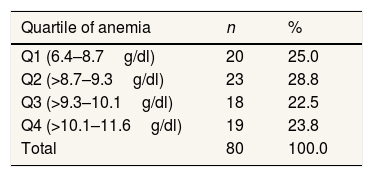
Quartile values from the results of hemoglobin examinations in pregnant women are divided into four sections, calculated by determining the median (middle value). Quartile 1 (Q1) with Hemoglobin (HB) level 6.4–8.7g/dl (20 pregnant women), Quartile 2 (Q2) with HB level >8.7–9.3g/dl (23 pregnant women), Q3 with HB level >9.3–10.1g/dl (18 pregnant women) and Q4 >10.1–11.6g/dl (19 pregnant women).
ResultsThe results of this study are presented in the following Table 1.
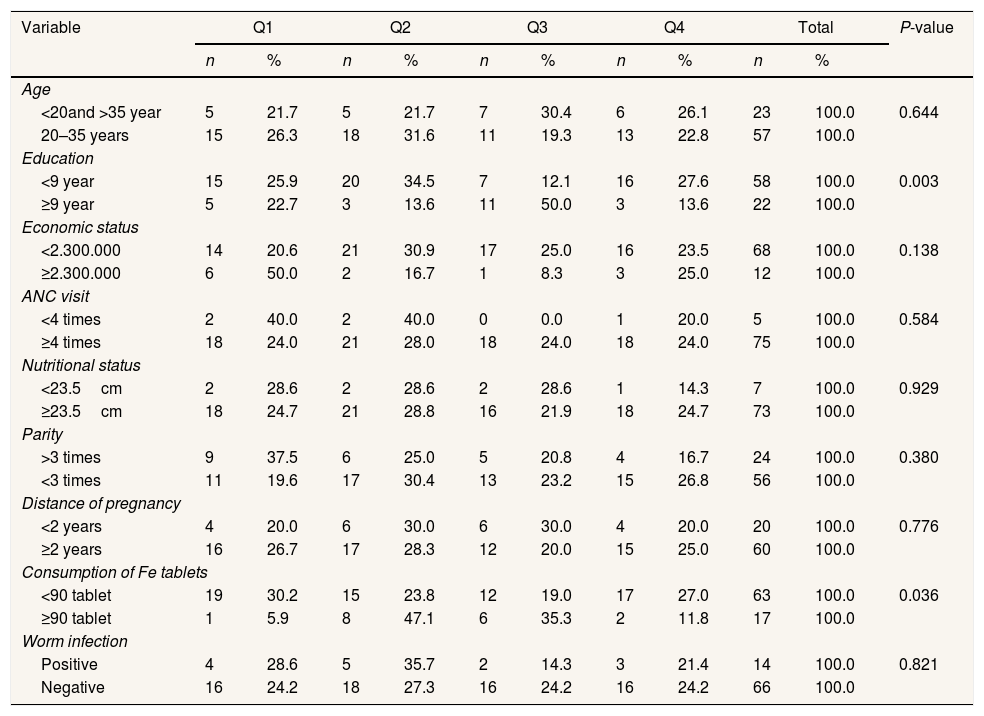
Table 1 shows that pregnant women in the study area mainly were in quartile 2, i.e., 23 pregnant women (28.8%). Based on the research results of the relationship between age and the incidence of anemia in pregnancy in a third-trimester pregnant woman, P-value=0.644, which means no significant relationship to anemia in pregnancy. The relationship between education and the incidence of anemia in pregnancy in the third trimester of pregnant women has obtained P-value=0.003, which means there is a significant relationship with anemia.
The relationship between the economic status and the incidence of anemia in pregnancy in the third trimester of pregnant women was obtained by P-value=0.138, which means no significant relationship to anemia in pregnancy. Likewise, the relationship between antenatal care visits to the incidence of anemia in pregnancy in the third trimester of pregnant women is obtained by P-value=0.584, which means no significant relationship to anemia. Finally, the relationship between the nutritional status and the incidence of anemia in pregnancy in the third-trimester pregnant women obtained P-value=0.929, which means no significant relationship to anemia.
The relationship between parity and incidence of anemia in pregnancy in the third trimester of pregnant women obtained a P-value of 0.380, indicating no significant relationship to anemia. The relationship between the distance of pregnancy with the incidence of anemia in pregnancy in the third trimester of pregnant women has obtained a P-value value of 0.776, which means no significant relationship to anemia. The relationship between the consumption of iron tablets with the incidence of anemia in pregnancy in the Third-trimester of pregnant women obtained the value of P-value=0.036, which means there is a significant relationship to anemia. The relationship between worm infection and anemia incidence in pregnancy in third-trimesters of pregnant women obtained a P-value of 0.821, which means no significant relationship to anemia (Table 2).
Determinant of anemia in pregnancy.
| Variable | Q1 | Q2 | Q3 | Q4 | Total | P-value | |||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| n | % | n | % | n | % | n | % | n | % | ||
| Age | |||||||||||
| <20and >35 year | 5 | 21.7 | 5 | 21.7 | 7 | 30.4 | 6 | 26.1 | 23 | 100.0 | 0.644 |
| 20–35 years | 15 | 26.3 | 18 | 31.6 | 11 | 19.3 | 13 | 22.8 | 57 | 100.0 | |
| Education | |||||||||||
| <9 year | 15 | 25.9 | 20 | 34.5 | 7 | 12.1 | 16 | 27.6 | 58 | 100.0 | 0.003 |
| ≥9 year | 5 | 22.7 | 3 | 13.6 | 11 | 50.0 | 3 | 13.6 | 22 | 100.0 | |
| Economic status | |||||||||||
| <2.300.000 | 14 | 20.6 | 21 | 30.9 | 17 | 25.0 | 16 | 23.5 | 68 | 100.0 | 0.138 |
| ≥2.300.000 | 6 | 50.0 | 2 | 16.7 | 1 | 8.3 | 3 | 25.0 | 12 | 100.0 | |
| ANC visit | |||||||||||
| <4 times | 2 | 40.0 | 2 | 40.0 | 0 | 0.0 | 1 | 20.0 | 5 | 100.0 | 0.584 |
| ≥4 times | 18 | 24.0 | 21 | 28.0 | 18 | 24.0 | 18 | 24.0 | 75 | 100.0 | |
| Nutritional status | |||||||||||
| <23.5cm | 2 | 28.6 | 2 | 28.6 | 2 | 28.6 | 1 | 14.3 | 7 | 100.0 | 0.929 |
| ≥23.5cm | 18 | 24.7 | 21 | 28.8 | 16 | 21.9 | 18 | 24.7 | 73 | 100.0 | |
| Parity | |||||||||||
| >3 times | 9 | 37.5 | 6 | 25.0 | 5 | 20.8 | 4 | 16.7 | 24 | 100.0 | 0.380 |
| <3 times | 11 | 19.6 | 17 | 30.4 | 13 | 23.2 | 15 | 26.8 | 56 | 100.0 | |
| Distance of pregnancy | |||||||||||
| <2 years | 4 | 20.0 | 6 | 30.0 | 6 | 30.0 | 4 | 20.0 | 20 | 100.0 | 0.776 |
| ≥2 years | 16 | 26.7 | 17 | 28.3 | 12 | 20.0 | 15 | 25.0 | 60 | 100.0 | |
| Consumption of Fe tablets | |||||||||||
| <90 tablet | 19 | 30.2 | 15 | 23.8 | 12 | 19.0 | 17 | 27.0 | 63 | 100.0 | 0.036 |
| ≥90 tablet | 1 | 5.9 | 8 | 47.1 | 6 | 35.3 | 2 | 11.8 | 17 | 100.0 | |
| Worm infection | |||||||||||
| Positive | 4 | 28.6 | 5 | 35.7 | 2 | 14.3 | 3 | 21.4 | 14 | 100.0 | 0.821 |
| Negative | 16 | 24.2 | 18 | 27.3 | 16 | 24.2 | 16 | 24.2 | 66 | 100.0 | |
*Chi-square.
Q (quartile).
Low education of pregnant women will have an impact on insufficient knowledge. The low level of maternal education affects the acceptance of information, so knowledge of iron is limited.6,7 According to the researcher, the higher the level of education of a person, the easier it is to receive information so that more knowledge will be possessed both in the prevention of anemia in pregnancy, in fulfilling the nutritional needs of pregnant women, and in the utilization of existing health services. The theory above is in line with the results of this study, which found significant results for the incidence of anemia in pregnancy, namely P-value=0.003. This is because the number of pregnant women with low education has more anemia than highly educated pregnant women. In addition, pregnant women who rarely consume Fe tablets are more likely to experience anemia if they are not balanced by iron-containing.
ConclusionIn this study of 80 third-trimester pregnant women, 75 people (93.8%) pregnant women had anemia, and five people (6.8%) were pregnant women who did not experience anemia. The results showed that two determinant variables significantly affected anemia in pregnancy, namely education and consumption of iron tablets, and seven other determinants did not significantly influence the incidence of anemia in pregnancy, namely age, education, economic status, antenatal care visit, nutritional status, parity, the distance between pregnancy and worm infection in the Polewali Mandar district.
Conflicts of interestThe authors declare no conflict of interest.
Peer-review under responsibility of the scientific committee of the 3rd International Nursing, Health Science Students & Health Care Professionals Conference. Full-text and the content of it is under responsibility of authors of the article.











