



To examine relevant differences in the prevalence of overweight and obesity in children aged 2-15 years according to different sets of criteria (Orbegozo Foundation, International Obesity Task Force and World Health Organization), and how their use affects the trends in obesity recorded for both sexes between 1995 and 2011 in Spain.
MethodCross-sectional study, a population between 2 and 15 years. Three diagnosis criteria of overweight and obesity were be used.
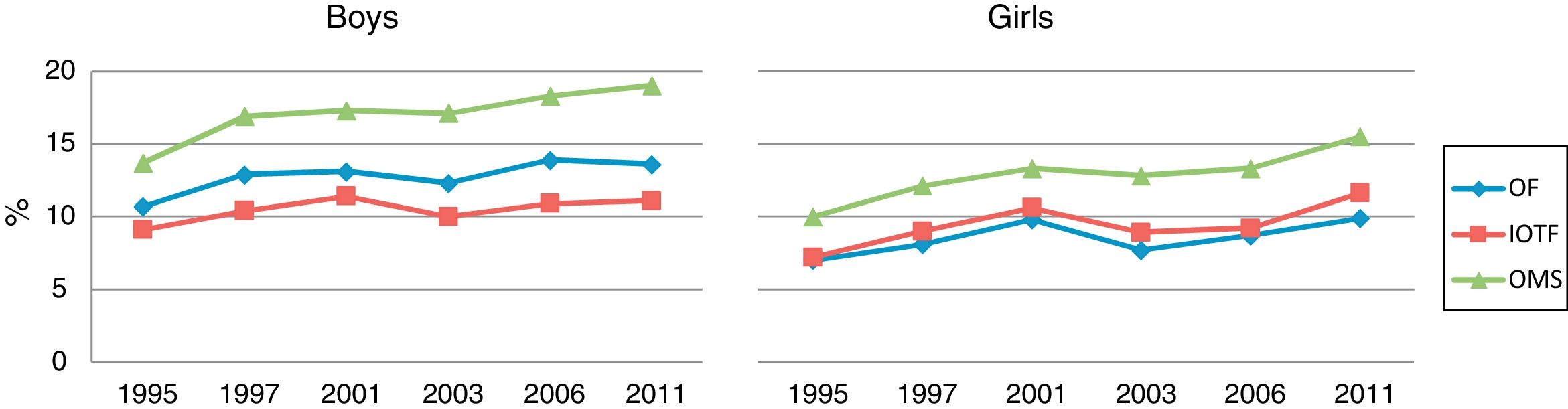
ResultsThe boys according to the three criteria, showed higher values of overweight and obesity compared to the girls. The lowest levels of overweight and obesity were observed using the Orbegozo tables.
DiscussionThe prevalence of overweight and obesity varies significantly according to the criteria used to define overweight and obesity. The percentiles of the Foundation Orbegozo gave the lowest estimates and the standards of growth of the World Health Organization were higher.
Evaluar si existen diferencias relevantes entre los valores de prevalencia de sobrepeso y obesidad infantil en función de los tipos de criterios utilizados (Fundación Orbegozo, International Obesity Task Force, Organización Mundial de la Salud), y el modo en que su uso afecta a las tendencias sobre obesidad registradas para ambos sexos en España entre 2005 y 2011.
MétodoEstudio transversal, en una población de entre 2 y 15 años de edad. Se usaron tres criterios diagnósticos de sobrepeso y obesidad.
ResultadosLos niños, según los tres criterios utilizados, presentaron valores superiores de sobrepeso y obesidad en comparación con las niñas. Las cifras más bajas de sobrepeso y obesidad se observaron al emplear las tablas de Orbegozo.
DiscusiónLas prevalencias de sobrepeso y obesidad varían de manera significativa según los criterios utilizados para definir sobrepeso y obesidad. Los percentiles de la Fundación Orbegozo proporcionan las estimaciones más bajas, y los estándares de crecimiento de la Organización Mundial de la Salud las más altas.
Obesity, which the World Health Organisation (WHO) refers to as a ‘21st century epidemic’, is an increasingly important problem worldwide. Early diagnosis is vital in the prevention of its associated morbidity.
Despite their limitations, growth curves based on body mass index (BMI) are the tools most often used in epidemiological studies and screening programmes for determining childhood overweight-obesity. Indeed, their use is recommended by different expert groups.1 However, no consensus exists that might allow the establishment of unified diagnostic criteria for childhood obesity. Indeed, several institutions have established cut-offs in the hope of reaching agreement. The choice of reference curve is, of course, of great importance; a child of a particular sex, age and BMI might be classified as obese by one, but not by another2 Two of the most commonly used sets of criteria for establishing obesity are those of the International Obesity Task Force (IOTF)3 and the 2006 and 2007 criteria of the WHO for children aged 0-5 years and 5-19 years respectively.4 Another criteria is Orbegozo Foundation (OF), used in Spain.5,6
The aim of the present work was to examine the differences in the prevalence of overweight and obesity in children aged 2-15 years arising from the use of different sets of criteria (OF, IOTF and WHO), and how their use affects the trends in obesity recorded for both sexes between 1995 and 2011 in Spain.
MethodsInformation in the Spanish National Health Survey (ENS, Encuesta Nacional de Salud) (1995, 1997, 2001, 2003, 2006 and 2011) was examined in this cross-sectional descriptive study. The ENS is a survey performed in Spain that gathers data on health and the factors that determine its quality. It provides information on perceived morbidity, lifestyle, habits related to risk factors, the use of health services, and preventive practices. It also allows data to be collected from people who have not recently used any health service. The surveyed population is selected by stratified multistage sampling.7
The present work examined data for the population aged 2-15 years between 1995 and 2011. Information was collected on the body weight, height and sex of the respondents, the BMI of each calculated, and the prevalence of overweight and obesity determined for girls (n=11,663) and boys (n=11,574) (with their 95% confidence intervals) according to three sets of criteria: a) OF tables for the body weight of Spanish children;5b) the IOTF criteria, used the percentiles values in children, with the aim of establishing pediatric breakpoints;3 and c) the WHO growth standards for 2006/2007, which describe how much children ought to weigh between birth and adolescence.4 The prevalence values obtained were then compared using the McNemar test. Significance was set at p ≤0.05. All calculations were made using SPSS v.21.0 software for Windows.
Data were collected from secondary sources (public and anonymised data). It was not necessary to obtain the approval of Research Ethics Committee, according to Spanish law. Also, different national health surveys that were used as a secondary data source, had already obtained the permission of the Committee.
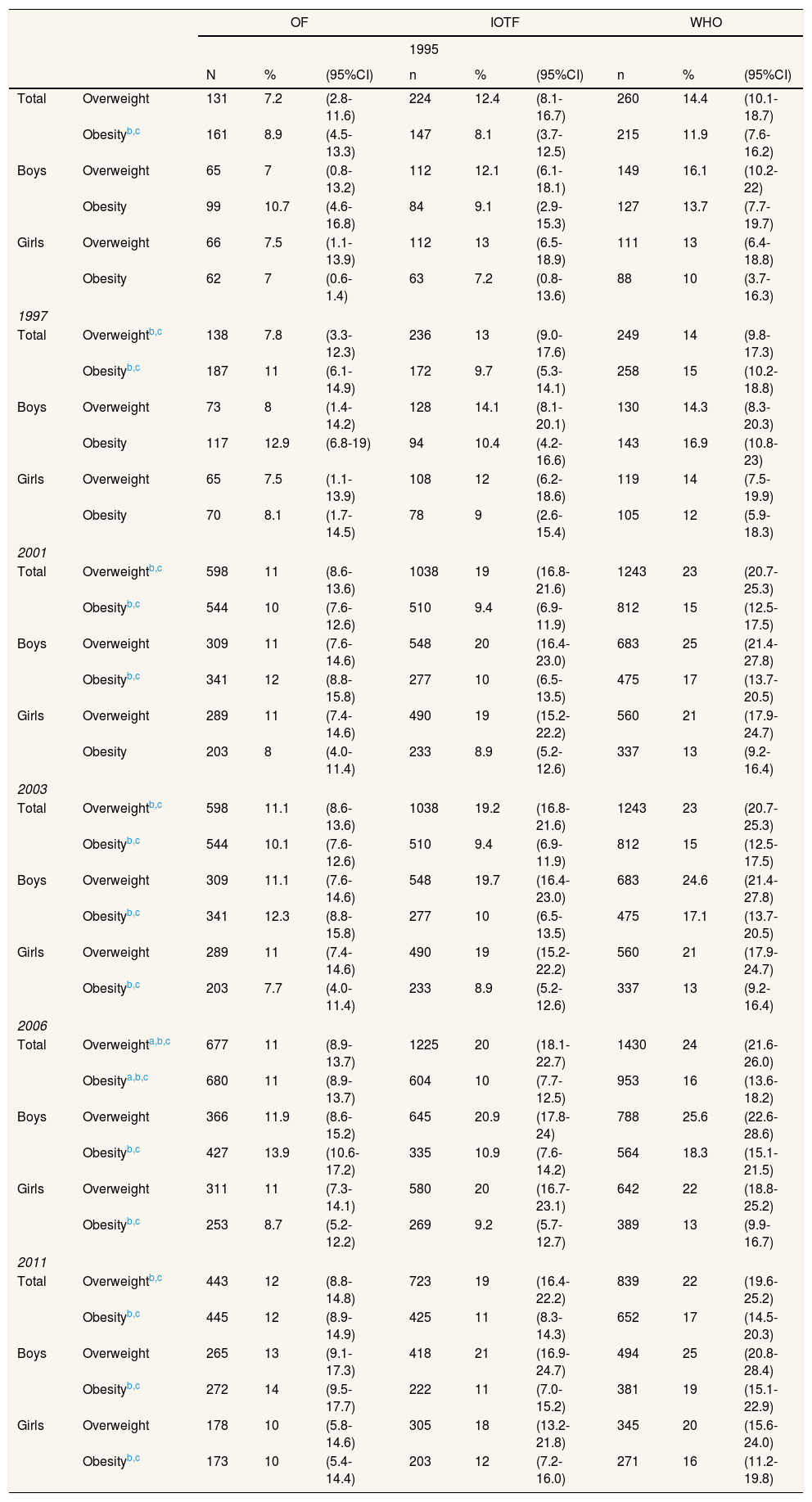
ResultsTable 1 shows the results obtained. According to all three sets of criteria, overweight and obesity were nearly always more common among the boys (obesity 1995: 13.7%; 2011: 19.0%) than among the girls (obesity 1995: 10.0%; 2011: 16.0%). The lowest prevalence values for overweight were recorded when using the OF tables (OF 12.0%, IOTF 19.0%, WHO 22.0%), while the lowest for obesity were obtained when using the IOFT criteria (OF 12.0%, IOTF 11.0%, WHO 17.0%). The WHO criteria consistently returned significantly higher overweight and obesity prevalence values for both girls and boys.
Prevalence of overweight and obesity in Spanish children according to the set of diagnostic criteria used.
| OF | IOTF | WHO | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| 1995 | ||||||||||
| N | % | (95%CI) | n | % | (95%CI) | n | % | (95%CI) | ||
| Total | Overweight | 131 | 7.2 | (2.8-11.6) | 224 | 12.4 | (8.1-16.7) | 260 | 14.4 | (10.1-18.7) |
| Obesityb,c | 161 | 8.9 | (4.5-13.3) | 147 | 8.1 | (3.7-12.5) | 215 | 11.9 | (7.6-16.2) | |
| Boys | Overweight | 65 | 7 | (0.8-13.2) | 112 | 12.1 | (6.1-18.1) | 149 | 16.1 | (10.2-22) |
| Obesity | 99 | 10.7 | (4.6-16.8) | 84 | 9.1 | (2.9-15.3) | 127 | 13.7 | (7.7-19.7) | |
| Girls | Overweight | 66 | 7.5 | (1.1-13.9) | 112 | 13 | (6.5-18.9) | 111 | 13 | (6.4-18.8) |
| Obesity | 62 | 7 | (0.6-1.4) | 63 | 7.2 | (0.8-13.6) | 88 | 10 | (3.7-16.3) | |
| 1997 | ||||||||||
| Total | Overweightb,c | 138 | 7.8 | (3.3-12.3) | 236 | 13 | (9.0-17.6) | 249 | 14 | (9.8-17.3) |
| Obesityb,c | 187 | 11 | (6.1-14.9) | 172 | 9.7 | (5.3-14.1) | 258 | 15 | (10.2-18.8) | |
| Boys | Overweight | 73 | 8 | (1.4-14.2) | 128 | 14.1 | (8.1-20.1) | 130 | 14.3 | (8.3-20.3) |
| Obesity | 117 | 12.9 | (6.8-19) | 94 | 10.4 | (4.2-16.6) | 143 | 16.9 | (10.8-23) | |
| Girls | Overweight | 65 | 7.5 | (1.1-13.9) | 108 | 12 | (6.2-18.6) | 119 | 14 | (7.5-19.9) |
| Obesity | 70 | 8.1 | (1.7-14.5) | 78 | 9 | (2.6-15.4) | 105 | 12 | (5.9-18.3) | |
| 2001 | ||||||||||
| Total | Overweightb,c | 598 | 11 | (8.6-13.6) | 1038 | 19 | (16.8-21.6) | 1243 | 23 | (20.7-25.3) |
| Obesityb,c | 544 | 10 | (7.6-12.6) | 510 | 9.4 | (6.9-11.9) | 812 | 15 | (12.5-17.5) | |
| Boys | Overweight | 309 | 11 | (7.6-14.6) | 548 | 20 | (16.4-23.0) | 683 | 25 | (21.4-27.8) |
| Obesityb,c | 341 | 12 | (8.8-15.8) | 277 | 10 | (6.5-13.5) | 475 | 17 | (13.7-20.5) | |
| Girls | Overweight | 289 | 11 | (7.4-14.6) | 490 | 19 | (15.2-22.2) | 560 | 21 | (17.9-24.7) |
| Obesity | 203 | 8 | (4.0-11.4) | 233 | 8.9 | (5.2-12.6) | 337 | 13 | (9.2-16.4) | |
| 2003 | ||||||||||
| Total | Overweightb,c | 598 | 11.1 | (8.6-13.6) | 1038 | 19.2 | (16.8-21.6) | 1243 | 23 | (20.7-25.3) |
| Obesityb,c | 544 | 10.1 | (7.6-12.6) | 510 | 9.4 | (6.9-11.9) | 812 | 15 | (12.5-17.5) | |
| Boys | Overweight | 309 | 11.1 | (7.6-14.6) | 548 | 19.7 | (16.4-23.0) | 683 | 24.6 | (21.4-27.8) |
| Obesityb,c | 341 | 12.3 | (8.8-15.8) | 277 | 10 | (6.5-13.5) | 475 | 17.1 | (13.7-20.5) | |
| Girls | Overweight | 289 | 11 | (7.4-14.6) | 490 | 19 | (15.2-22.2) | 560 | 21 | (17.9-24.7) |
| Obesityb,c | 203 | 7.7 | (4.0-11.4) | 233 | 8.9 | (5.2-12.6) | 337 | 13 | (9.2-16.4) | |
| 2006 | ||||||||||
| Total | Overweighta,b,c | 677 | 11 | (8.9-13.7) | 1225 | 20 | (18.1-22.7) | 1430 | 24 | (21.6-26.0) |
| Obesitya,b,c | 680 | 11 | (8.9-13.7) | 604 | 10 | (7.7-12.5) | 953 | 16 | (13.6-18.2) | |
| Boys | Overweight | 366 | 11.9 | (8.6-15.2) | 645 | 20.9 | (17.8-24) | 788 | 25.6 | (22.6-28.6) |
| Obesityb,c | 427 | 13.9 | (10.6-17.2) | 335 | 10.9 | (7.6-14.2) | 564 | 18.3 | (15.1-21.5) | |
| Girls | Overweight | 311 | 11 | (7.3-14.1) | 580 | 20 | (16.7-23.1) | 642 | 22 | (18.8-25.2) |
| Obesityb,c | 253 | 8.7 | (5.2-12.2) | 269 | 9.2 | (5.7-12.7) | 389 | 13 | (9.9-16.7) | |
| 2011 | ||||||||||
| Total | Overweightb,c | 443 | 12 | (8.8-14.8) | 723 | 19 | (16.4-22.2) | 839 | 22 | (19.6-25.2) |
| Obesityb,c | 445 | 12 | (8.9-14.9) | 425 | 11 | (8.3-14.3) | 652 | 17 | (14.5-20.3) | |
| Boys | Overweight | 265 | 13 | (9.1-17.3) | 418 | 21 | (16.9-24.7) | 494 | 25 | (20.8-28.4) |
| Obesityb,c | 272 | 14 | (9.5-17.7) | 222 | 11 | (7.0-15.2) | 381 | 19 | (15.1-22.9) | |
| Girls | Overweight | 178 | 10 | (5.8-14.6) | 305 | 18 | (13.2-21.8) | 345 | 20 | (15.6-24.0) |
| Obesityb,c | 173 | 10 | (5.4-14.4) | 203 | 12 | (7.2-16.0) | 271 | 16 | (11.2-19.8) | |
95%CI: 95% confidence interval; IOTF: International Obesity Task Force; OF: Orbegozo Foundation; WHO: World Health Organization.
Figure 1 shows all criteria sets to report a rising trend in obesity for both sexes between 1995 and 2003, then a small fall before rising again until 2011.
Discussion
The results show that the diagnostic criteria used to determine the prevalence of overweight and obesity can strongly affect the values obtained. The same child might be deemed of normal weight by one set of criteria, yet obese by another. If different sets of criteria are used, confusion can arise when examining trends over time or differences between regions or countries. Certainly, there are more than the three sets of criteria used in the present work, including those developed in the Enkid study,8 those reported by Carrascosa,9 and the two sets provided by the OF (19885 and 20116). OF 1988 was used to monitor the growth and detect changes in its evolution. Moreover, the study is longitudinal as the WHO and IOTF criteria. FO 2011 criteria brings data from a cross-sectional study. So, the comparison of the results is difficult. In the USA, the criteria issued by the Centers for Disease Control are those most commonly used, but the information on which they are based is not representative of all countries; they cannot, therefore, be safely used outside the USA. Certainly, children deemed obese in some countries would be thought of normal weight in North America.10
Attempts have been made to solve the problems this causes in epidemiological studies when comparing countries with different ethnic and geographical characteristics. Indeed, in an initial proposal, the IOTF criteria were suggested for wider use,3 followed by the candidacy of WHO criteria.4 However, no international consensus exists regarding which criteria are best, and when nations use their own, home-developed rules, the complications only become worse.11,12 Recently, the ALADINO study undertaken by the Agencia Española de Consumo, Seguridad Alimentaria y Nutrición also reported large differences in the prevalence values obtained when using different criteria for overweight and obesity.13,14
It is therefore important that consensus be reached regarding the criteria defining overweight and obesity in children. If none is reached, it will remain very difficult to compare the results of different studies and even come to decisions regarding the interventions that may be required.15
All the criteria sets examined in the present work showed a rise in the prevalence of obesity over the study period. According to the WHO criteria, which consistently returned the highest results, the prevalence of childhood obesity was lower between 1995 and 2003, at 11.9% and 15% respectively, rising to 17% by 2011. The results of the World Obesity Federation15 agree with this finding. For example, Australia experienced a rise in childhood obesity from 11% in 1985 to 21% in 2008; in England, 9% of children were obese in 1974 compared to 25% in 2002; in Iceland, a rise was seen from 9% in 1969 to 24% in 1998; and in Scotland an increase was recorded from 9% in 1974 to 24% in 2010.
So, the WHO criteria are better than OF or IOTF because their international applicability and their methodological quality.
The use of different criteria may produce negative consequences at individual and institutional level. An increased in morbidity is produced if the diagnosis and treatment delayed. In relation to public policies would increases consumption of human and material resources.
In conclusion, the prevalence values for overweight and obesity in children may vary widely depending on the criteria used to define these conditions. The present work showed the WHO criteria set to return the highest values for both variables, both in boys and girls. This hinders the comparison of different studies, highlighting the need to formulate consensus criteria. Between 1995 and 2011, Spain experienced a trend towards a greater prevalence in childhood obesity (as shown by all criteria sets), highlighting the need to control this 21st century epidemic.
Editor in chargeLaura I. González Zapata.
Transparency declarationThe corresponding author on behalf of the other authors guarantee the accuracy, transparency and honesty of the data and information contained in the study, that no relevant information has been omitted and that all discrepancies between authors have been adequately resolved and described.
Obesity has reached epidemic proportions in many parts of the world; the WHO refers to it as a 21st century epidemic. Studies on the prevalence of child overweight and obesity in Spain have suggested different results may be returned depending on the criteria used to define these conditions.
What does this study add to the literature?This work confirms that the use of different criteria sets for overweight-obesity can significantly affect the prevalence values obtained for these conditions. The criteria set proposed by the WHO was found to consistently return higher prevalence values for both conditions than those proposed by the International Obesity Task Force or Orbegozo Foundation. The use of different criteria sets makes it difficult to compare the results of different studies and different populations.
All authors participated in the conception and design of the study. Ajejas Bazán MJ, Jiménez Trujillo MI, and Pérez Farinós N performed the analysis and interpretation of the data. Wärnberg J and Domínguez Fernández S conducted a critical review of the results obtained and data analysis. All authors participated in the drafting of the manuscript and approved its final version.
FundingNone.
Conflicts of interestNone.











