



The proverb “Words are like cherries”, meaning that when you start talking subjects pop up and you end up with long conversations, just like cherries coming out of the plate in chains when you pick one, may also be applied to epidemiological research. A sequence of epidemiological studies, each being drawn from the previous, is presented as an example of how each investigation may raise new questions to be addressed in following studies.
This description stresses the need for appropriate planning and the usefulness of pilot testing to depict inadequacies that can hardly be anticipated without field work. I intend to illustrate how epidemiological research can provide a deep approach to research questions, as long as findings are properly interpreted and suboptimal methodological options are taken into account in future investigations.
El proverbio “Las palabras son como las cerezas” que expresa cómo cuando empezamos a hablar los asuntos van surgiendo de manera encadenada y terminamos con largas conversaciones, del mismo modo en que las cerezas que salen del plato encadenadas cuando cogemos una, puede también puede ser aplicado a la investigación epidemiológica. Una secuencia de estudios epidemiológicos, cada uno derivado del anterior, se presenta como un ejemplo de cómo cada investigación puede derivar en nuevas cuestiones en los estudios siguientes.
Esta descripción subraya la necesidad de una planificación adecuada así como la utilidad de los estudios piloto para describir las deficiencias que difícilmente podrían haber sido anticipadas sin trabajo de campo. Se pretende ilustrar como la investigación epidemiológica puede proporcionar un enfoque profundo a cuestiones de investigación, siempre y cuando los resultados sean interpretados correctamente y las opciones metodológicas subóptimas sean tenidas en cuenta en futuras investigaciones.
In this field note I present a set of original results, preceded by the chain of reasoning that brought us to them, and followed by the research that was subsequently generated.
The seed for the described investigations was a survey conducted in Portugal, aiming to quantify the prevalence of drug allergy in University students, which allowed us to fill a gap in the knowledge of the descriptive epidemiology of drug allergy in our population.1 We had the opportunity to replicate this study in Mozambique, motivated by the novelty of such data in the African setting.2 The questionnaire was carefully adapted to the local specificities, but we were surprised by an 18% prevalence of self-reported chloroquine allergy in the black population. (Table 1).
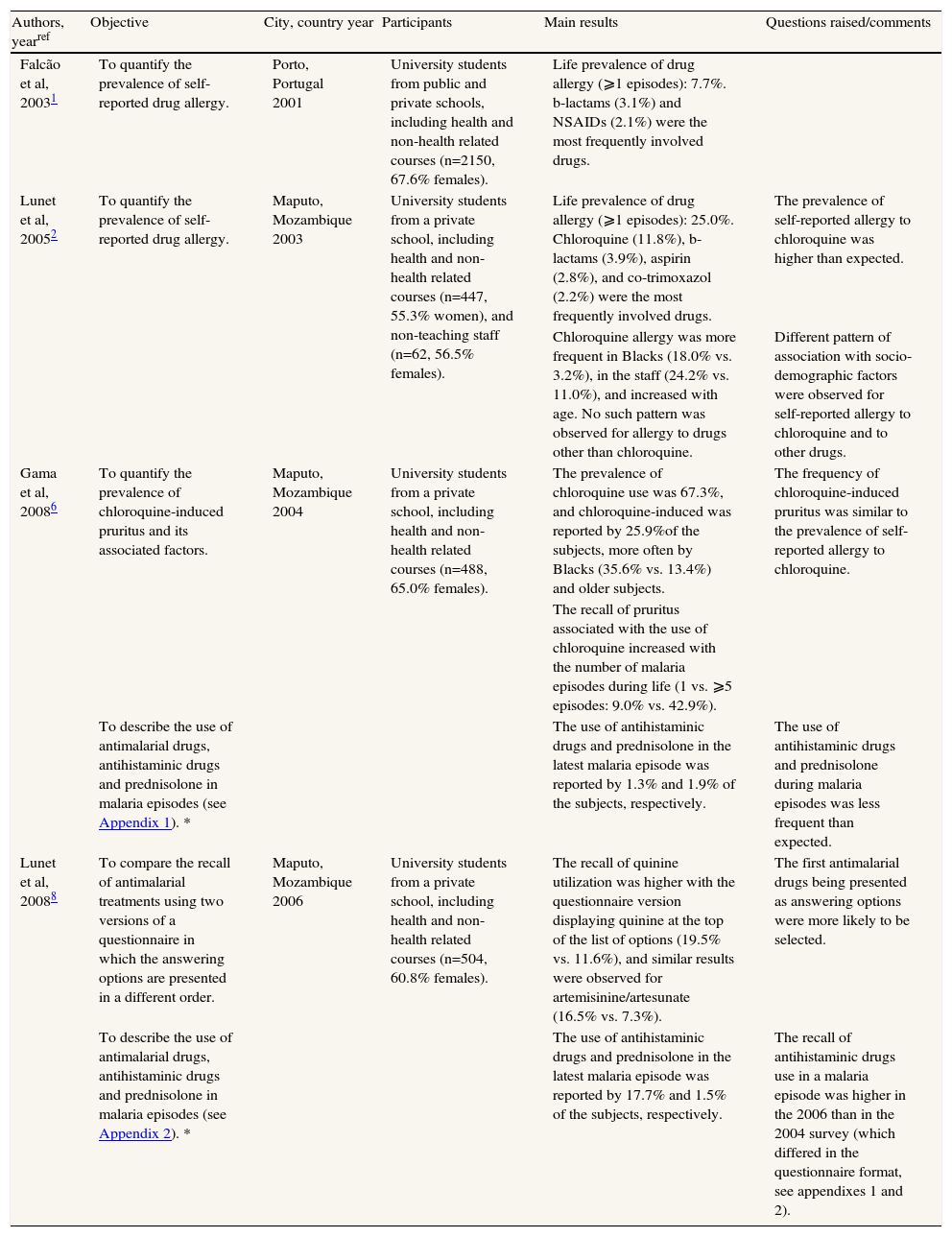
Main characteristics and results of the studies presented in this report
| Authors, yearref | Objective | City, country year | Participants | Main results | Questions raised/comments |
| Falcão et al, 20031 | To quantify the prevalence of self-reported drug allergy. | Porto, Portugal 2001 | University students from public and private schools, including health and non-health related courses (n=2150, 67.6% females). | Life prevalence of drug allergy (⩾1 episodes): 7.7%. b-lactams (3.1%) and NSAIDs (2.1%) were the most frequently involved drugs. | |
| Lunet et al, 20052 | To quantify the prevalence of self-reported drug allergy. | Maputo, Mozambique 2003 | University students from a private school, including health and non-health related courses (n=447, 55.3% women), and non-teaching staff (n=62, 56.5% females). | Life prevalence of drug allergy (⩾1 episodes): 25.0%. Chloroquine (11.8%), b-lactams (3.9%), aspirin (2.8%), and co-trimoxazol (2.2%) were the most frequently involved drugs. | The prevalence of self-reported allergy to chloroquine was higher than expected. |
| Chloroquine allergy was more frequent in Blacks (18.0% vs. 3.2%), in the staff (24.2% vs. 11.0%), and increased with age. No such pattern was observed for allergy to drugs other than chloroquine. | Different pattern of association with socio-demographic factors were observed for self-reported allergy to chloroquine and to other drugs. | ||||
| Gama et al, 20086 | To quantify the prevalence of chloroquine-induced pruritus and its associated factors. | Maputo, Mozambique 2004 | University students from a private school, including health and non-health related courses (n=488, 65.0% females). | The prevalence of chloroquine use was 67.3%, and chloroquine-induced was reported by 25.9%of the subjects, more often by Blacks (35.6% vs. 13.4%) and older subjects. | The frequency of chloroquine-induced pruritus was similar to the prevalence of self-reported allergy to chloroquine. |
| The recall of pruritus associated with the use of chloroquine increased with the number of malaria episodes during life (1 vs. ⩾5 episodes: 9.0% vs. 42.9%). | |||||
| To describe the use of antimalarial drugs, antihistaminic drugs and prednisolone in malaria episodes (see Appendix 1). * | The use of antihistaminic drugs and prednisolone in the latest malaria episode was reported by 1.3% and 1.9% of the subjects, respectively. | The use of antihistaminic drugs and prednisolone during malaria episodes was less frequent than expected. | |||
| Lunet et al, 20088 | To compare the recall of antimalarial treatments using two versions of a questionnaire in which the answering options are presented in a different order. | Maputo, Mozambique 2006 | University students from a private school, including health and non-health related courses (n=504, 60.8% females). | The recall of quinine utilization was higher with the questionnaire version displaying quinine at the top of the list of options (19.5% vs. 11.6%), and similar results were observed for artemisinine/artesunate (16.5% vs. 7.3%). | The first antimalarial drugs being presented as answering options were more likely to be selected. |
| To describe the use of antimalarial drugs, antihistaminic drugs and prednisolone in malaria episodes (see Appendix 2). * | The use of antihistaminic drugs and prednisolone in the latest malaria episode was reported by 17.7% and 1.5% of the subjects, respectively. | The recall of antihistaminic drugs use in a malaria episode was higher in the 2006 than in the 2004 survey (which differed in the questionnaire format, see appendixes 1 and 2). |
The objectives signed with * are addressed in this report, but were not explored in the previously published articles.
NSAIDs-non-steroidal anti-inflammatory drugs.
No similar studies from malaria endemic or epidemic countries had been published before, but in the large number of citizens from developed countries exposed to chloroquine for malaria chemoprophylaxis, chloroquine has never been described as having a strong allergenic potential. On the other hand, chloroquine-induced pruritus, apparently a non IgE-mediated condition, has been described as frequent in black subjects, compromising treatment adherence.3,4 Evidence of the resurgence of chloroquine-susceptible falciparum malaria about a decade after its withdrawal5 resulted in boosted relevance for issues related to the appropriateness of chloroquine use.
Taking advantage of the ethnic diversity of the Mozambican population, we conducted a new cross sectional study, in 2004, ultimately aiming to understand the dose-response relation between chloroquine use and pruritus and the effect of this common side effect on future treatment options.6 Also, local pharmacists had the perception that antihistaminic drugs or prednisolone were frequently used in association with chloroquine, in an attempt to minimize its associated pruritus, despite the lack of evidence for the benefit of such procedure. Therefore, we quantified the use of the different antimalarial drugs, antihistaminic drugs and prednisolone, as described below.
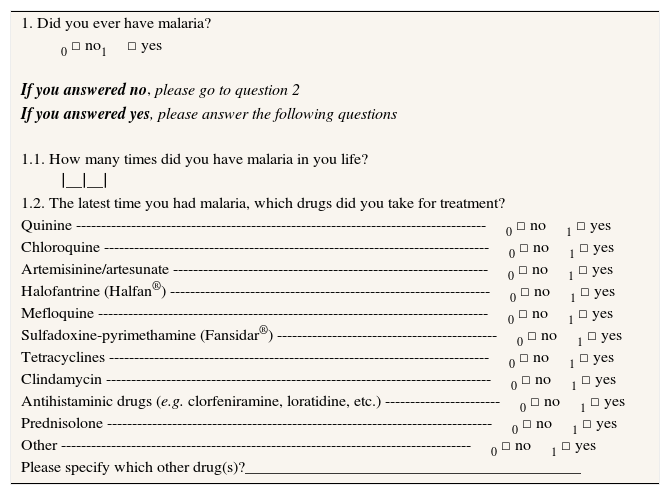
A self-administered questionnaire (Appendix 1) was used to collect information on the treatment of the latest malaria episode, when applicable. The pharmacological treatment was assessed by asking specifically for each of the antimalarial drugs available in Mozambique at that time, and the list of drugs also included the items “antihistaminic drugs (e.g. chlorpheniramine, loratadine, etc.)” and “prednisolone” (most drugs are well known by their generic name in this setting). Four hundred and eighty eight subjects were evaluated, representing approximately 50% of the total number of students in diurnal classes. Eighteen students (3.6%) refused to participate. Respondents’ median age was 21 years (range: 18 to 51 years), 65.0% were females, 29.9% attended health related courses, 73.5% had had malaria at least once.
The proportion of subjects reporting to have used chloroquine before was 67.3%, from which 25.9% reported episodes of intense pruritus associated with chloroquine, supporting the hypothesis that the terms “allergy” and “pruritus” may have been interpreted as interchangeable by the participants, which could explain the unexpectedly high prevalence of self-reported chloroquine allergy observed in the first survey. Further research, namely qualitative, could contribute to further understand this phenomenon.
Surprisingly, the use of antihistaminics and prednisolone in the latest malaria episode was reported by only 1.3% and 1.9%, respectively.
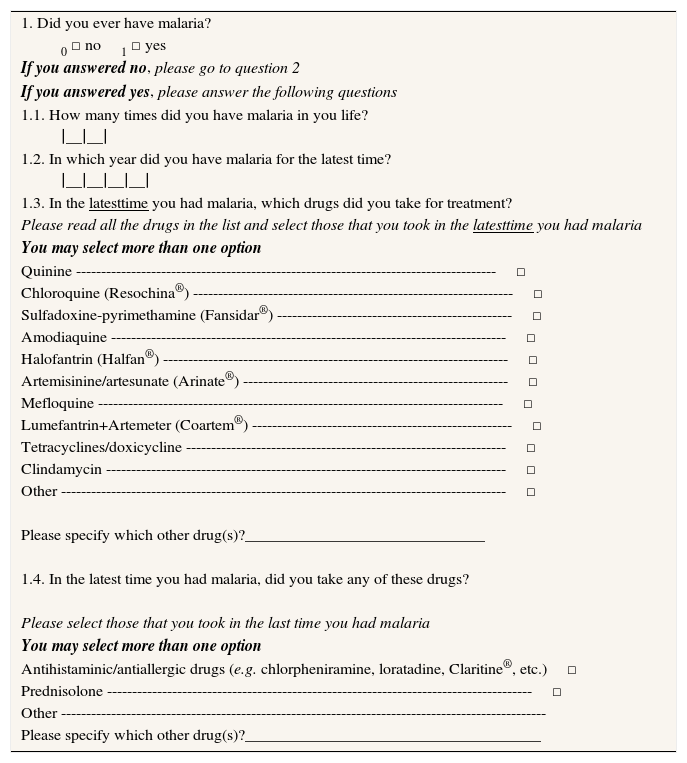
The more plausible explanation for these low prevalence estimates is the fact that the questionnaire referred to drugs used in the latest treatment for malaria, not distinguishing between antimalarial treatments and other drugs that could be used during a malaria episode, as it is know that more specific questions contribute to a better recall.7 This hypothesis was tested when the survey was repeated,8 two years later, using a questionnaire with separate headings for the antimalarial and for the drugs that could be used to relief pruritus (Appendix 2). The methods used and the population evaluated in the 2006 survey were similar to those in 2004. We evaluated 504 subjects, approximately 50% of the total number of students in the institution in diurnal classes. Fourteen students (2.7%) refused to participate. Respondents’ median age was 20 years (range: 18 to 57 years), 60.8% were females, 33.8% attended health related courses, and 72.6% had had malaria at least once. The proportion of drug use in 2004 and 2006 was compared with the χ2 test, or the Fisher exact test when appropriate.
The reported frequency of antihistaminic use during the latest malaria episode was substantially higher in the 2006 survey (17.7% vs. 1.3%, p<0.001), but no statistically significant differences were observed for prednisolone (1.5% vs. 1.9%, p=0.70). In the survey performed in 2006, the proportion of subjects using chloroquine in the treatment of malaria was 57% when the latest episode took place before 2004, and 42%, 18% and 12% in the episodes occurring in 2004, 2005 and 2006, respectively, reflecting the replacement of chloroquine by artemisin-based combination treatments as first-line therapy for falciparum malaria in all endemic areas in Africa. Among the subjects who had their latest malaria episode before 2004, the prevalence of antihistaminic drug use was 17.7%, and 2.3% of the participants used prednisolone in association with the antimalarial drugs.
The differences observed in responses to these two questionnaires of different structure are much larger than could be expected given the results from previous studies showing the variation in the completeness of ascertainment of drug exposure according to how the participants are questioned.7 We hypothesized that the underreporting could have been further increased by the fact that respondents tend to choose the first response options when questions are presented visually (as in self-administered questionnaires),9 since the drugs with no antimalarial effect were placed at the end of the list. We could expect that after selecting an antimalarial drug most subjects did not read the rest of the options. This hypothesis was also tested in the 2006 survey, using an experimental design8 to compare two alternative versions of the questionnaire, differing only in the order in which each proposed drug was presented in the response options (quinine and most frequently used drugs presented first vs. less frequently used drugs first and quinine at the end). This analysis showed that the first antimalarial drugs being presented as answering options were more likely to be selected.
Taken together, these results show that symptomatic treatment of itching is more likely to be recalled when a specific question is placed for antihistaminic drugs and most of the times ignored when the answering option for antihistaminic drugs is presented together with antimalarial drugs.
The proverb “Words are like cherries”, meaning that when you start talking subjects pop up and you end up with long conversations, just like cherries coming out of the plate in chains when you pick one, may also be applied to epidemiological research. Here I presented a sequence of epidemiological studies, each being drawn from the previous, as an example of how each investigation may raise new questions to be addressed in following studies.
To some extent, this example may be seen as an exercise of trial and error, which rarely can be conducted by a single researcher or research group due to the lengthy and complex nature of epidemiological research in general, stressing the need for in depth knowledge of the study subject, appropriate planning and pilot testing. The conduction of small-scale tests of the methods and procedures to be used on a larger scale epidemiological research10 is an important component of the research protocol, useful to depict inadequacies that can hardly be anticipated without field work.
This “chain” of studies, however, may also be described as an example of how epidemiological research can be conducted with reasonable depth, capitalizing a proper interpretation of the findings and the need to take consequences of suboptimal methodological options into account on new investigations.
Structure of the questionnaire used in the 2004 survey to evaluate malaria treatment (including antimalarial drugs, antihistaminic drugs, and prednisolone).
| 1. Did you ever have malaria? |
| 0 □ no1□ yes |
| If you answered no, please go to question 2 |
| If you answered yes, please answer the following questions |
| 1.1. How many times did you have malaria in you life? |
| ∣__∣__∣ |
| 1.2. The latest time you had malaria, which drugs did you take for treatment? |
| Quinine ----------------------------------------------------------------------------------0 □ no1 □ yes |
| Chloroquine -----------------------------------------------------------------------------0 □ no1 □ yes |
| Artemisinine/artesunate ---------------------------------------------------------------0 □ no1 □ yes |
| Halofantrine (Halfan®) ----------------------------------------------------------------0 □ no1 □ yes |
| Mefloquine ------------------------------------------------------------------------------0 □ no1 □ yes |
| Sulfadoxine-pyrimethamine (Fansidar®) --------------------------------------------0 □ no1 □ yes |
| Tetracyclines ----------------------------------------------------------------------------0 □ no1 □ yes |
| Clindamycin -----------------------------------------------------------------------------0 □ no1 □ yes |
| Antihistaminic drugs (e.g. clorfeniramine, loratidine, etc.) -----------------------0 □ no1 □ yes |
| Prednisolone -----------------------------------------------------------------------------0 □ no1 □ yes |
| Other ----------------------------------------------------------------------------------0 □ no1 □ yes |
| Please specify which other drug(s)?__________________________________________ |
Structure of the questionnaire used in the 2006 survey to evaluate malaria treatment (including antimalarial drugs and antipruritic drugs separately).
| 1. Did you ever have malaria? |
| 0 □ no1 □ yes |
| If you answered no, please go to question 2 |
| If you answered yes, please answer the following questions |
| 1.1. How many times did you have malaria in you life? |
| ∣__∣__∣ |
| 1.2. In which year did you have malaria for the latest time? |
| ∣__∣__∣__∣__∣ |
| 1.3. In the latesttime you had malaria, which drugs did you take for treatment? |
| Please read all the drugs in the list and select those that you took in the latesttime you had malaria |
| You may select more than one option |
| Quinine ------------------------------------------------------------------------------------□ |
| Chloroquine (Resochina®) ----------------------------------------------------------------□ |
| Sulfadoxine-pyrimethamine (Fansidar®) -----------------------------------------------□ |
| Amodiaquine -------------------------------------------------------------------------------□ |
| Halofantrin (Halfan®) ---------------------------------------------------------------------□ |
| Artemisinine/artesunate (Arinate®) -----------------------------------------------------□ |
| Mefloquine ---------------------------------------------------------------------------------□ |
| Lumefantrin+Artemeter (Coartem®) ----------------------------------------------------□ |
| Tetracyclines/doxicycline ----------------------------------------------------------------□ |
| Clindamycin --------------------------------------------------------------------------------□ |
| Other -----------------------------------------------------------------------------------------□ |
| Please specify which other drug(s)?______________________________ |
| 1.4. In the latest time you had malaria, did you take any of these drugs? |
| Please select those that you took in the last time you had malaria |
| You may select more than one option |
| Antihistaminic/antiallergic drugs (e.g. chlorpheniramine, loratadine, Claritine®, etc.)□ |
| Prednisolone -------------------------------------------------------------------------------------□ |
| Other ------------------------------------------------------------------------------------------------- |
| Please specify which other drug(s)?_____________________________________ |











