



To describe potential conditioning factors and to analyse improvement measures proposed by reporters in hospitals of an autonomous region of Spain.
MethodA cross-sectional study was conducted analysing all notifications from the public hospital network reported in Aragon (Spain) during 2023.
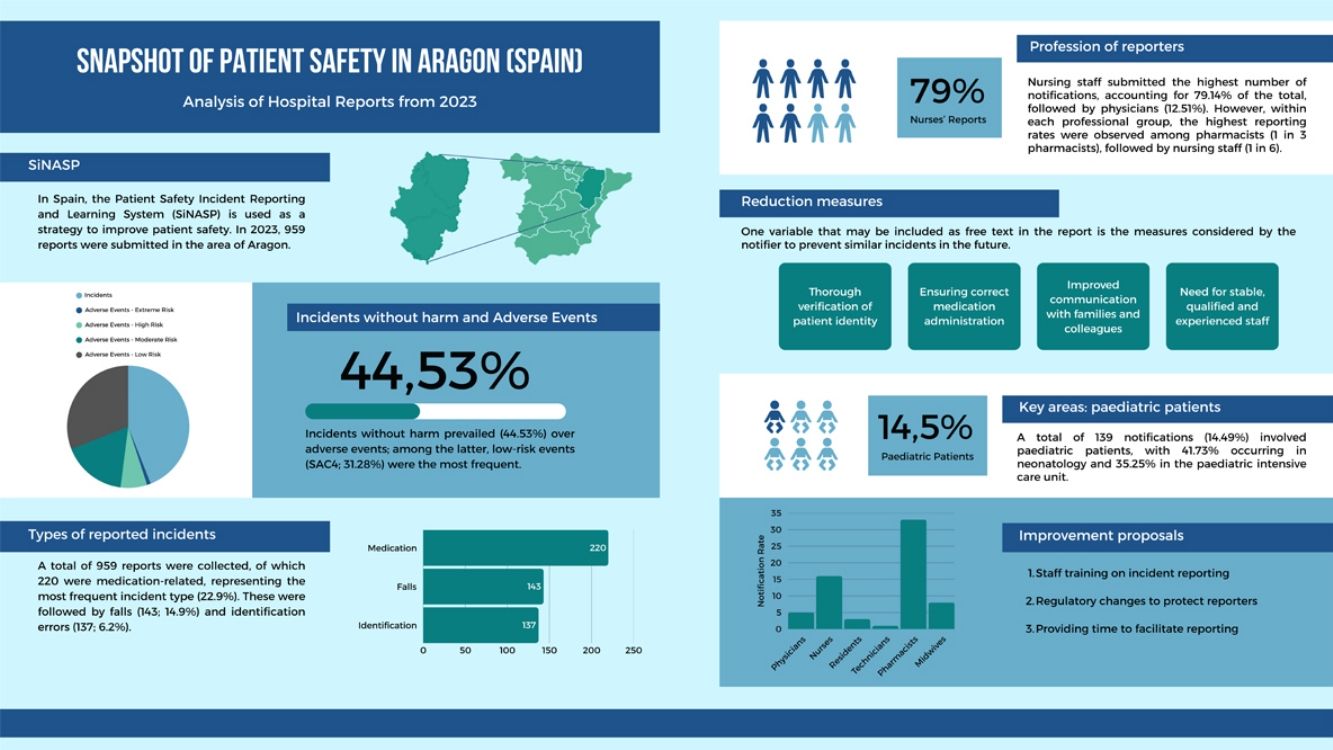
ResultsAmong all reports (n=959), incidents related to medication prevail (22.9%), followed by falls (14.9%) and identification issues (6.2%). Most of the reports were submitted by nurses (79.14%). Free text categories mainly indicated a need for improvements in terms of correct identification of patients and samples, both interpersonal and family communication, and a need of improvement in hospital staff stability and training.
ConclusionsDespite the limitations of the study, the main one being the voluntary and anonymous nature of the notification system, it presents a valuable source of knowledge to identify patient safety issues. In addition, following notifiers’ reports, it raises several important challenges, including better training for the notifying staff and the adoption of legal measures that guarantee the safety of the notifiers.
Describir los posibles factores condicionantes y analizar las medidas de mejora propuestas por los notificantes en los hospitales de Aragón.
MétodoMediante un estudio transversal se analizan todas las notificaciones de la red pública hospitalaria recogidas en Aragón durante el año 2023.
ResultadosEntre el total de las notificaciones (n=959) prevalecieron los incidentes relacionados con la medicación (22,9%), seguidos de las caídas (14,9%) y los problemas de identificación (6,2%). Predominaron las notificaciones realizadas por personal de enfermería (79,14%). En las categorías de texto libre se registró la necesidad de mejoras en términos de correcta identificación de pacientes y muestras, comunicación interpersonal y con los familiares, y mayor estabilidad y mejoría formativa del personal hospitalario.
ConclusionesA pesar de las limitaciones del estudio, siendo la principal el carácter voluntario y anónimo del sistema de notificación, este constituye una valiosa fuente de conocimiento para identificar problemas de seguridad del paciente. Además, a raíz de las propuestas de los notificantes, se plantean varios retos importantes, como una mejor formación del personal notificante y la adopción de medidas legales que garanticen su seguridad.

Patient safety encompasses different meanings and understandings, including: 1) the reduction of the risk of unnecessary harm related to health care to an acceptable minimum; 2) as a global strategy developed by health care organisations with the primary objective of minimising harm to patients; and 3) to describe the activities of identifying and analysing safety issues and managing risk in routine clinical practice. The risk of harm, known as hazard, is inherent in the provision of health care. It is increased by human error or system failures. Therefore, to provide quality health care, it is essential to try to avoid these risks and mitigate their impact on the patient.1
The World Health Organization (WHO) urges all countries to implement strategies to guarantee patient safety, considering it critical for health care quality and requiring both proactive and reactive risk management. Within this framework, the WHO defines within a standardised taxonomy: incidents related to patient safety are any event or circumstance that has caused or could have caused unnecessary harm to a patient; if it causes harm, it is called an adverse event. Contributing factors are circumstances, actions, or influences that play a role in the origin or evolution of an incident, or that increase the risk.2
When incidents or adverse events occur, their reporting is crucial for analysis, error correction, and prevention of recurrence. In Spain, Law 16/2003 on Cohesion and Quality of the National Health System already established the obligation of a registry of best practices and incidents. This mandate has been maintained in national and regional patient safety strategies, and in the Global Patient Safety Action Plan 2021-2030, which emphasises the importance of incident reporting and learning systems. Their importance is highlighted by the European Union and the Patient Safety Strategy of the Spanish National Health System for 2025-35.2–5
To improve patient safety, strategies are needed that make it possible to know: what is happening (research, surveillance, case analysis), what to do (evidence-based knowledge), and to verify whether it is applied (indicator monitoring).
Importance of notification systemsIn Spain, the Patient Safety Reporting and Learning System (SiNASP) was created with the objective of improving safety through the analysis of situations, problems, and incidents that caused or could have caused harm. This system produces annual reports for learning and improvement. Although SiNASP is widely implemented, it is not the only incident reporting system in Spain, as some autonomous regions have developed their own complementary systems (e.g. CISEMadrid in the Madrid region, notificASP in Andalusia, or SINEA in the Valencian region).6
Another approach to generating knowledge on patient safety in Spain has been through epidemiological studies designed to estimate the frequency and characteristics of adverse events across different healthcare settings (hospitals, primary care, etc.). In Spain, studies such as ENEAS (National Study on Hospitalisation-Related Adverse Events), APEAS (Patient Safety in Primary Health Care) and EARCAS (Patient Safety in Medical and Social Service Centres in Spain) are particularly relevant. These studies provide complementary information to incident reporting systems, as their methodologies and objectives differ, offering prevalence estimates and structured assessments of adverse events rather than voluntary incident reporting data.7
Other countries have implemented similar systems, such as the Australian Incident Monitoring System (AIMS) in Australia, the National Reporting & Learning System (NRLS) in the United Kingdom, and the Incident Reporting & Information System (IRIS), which differ in terms of anonymity, confidentiality, and mandatory reporting. Unlike countries such as Denmark or Italy, Spanish systems lack specific legal guarantees to protect reporting professionals. Denmark protects reporters from disciplinary consequences, keeping information separate from disciplinary systems and allowing anonymity. Italy, with the Gelli-Bianco Law (Law No. 24 of 2017) and the Stability Law (2015), prohibits the use of clinical risk management reports in judicial proceedings.8–11
SiNASP has undergone gradual development since its mandate in 2003, with pilot tests in 2009 and progressive implementation from 2010, extending to primary care in 2013. Its key principles include voluntary reporting, non-punitive character (separation from sanction systems), confidentiality, anonymous or nominative reporting with anonymisation, a systemic approach to examining contributing factors, and analysis for learning and implementation of improvements at the local level. The system covers near misses, no-harm incidents, and adverse events, excluding serious violations with obvious legal implications. The reporting process is carried out through an online portal, with sections to describe the incident, the patient, contributing factors, and risk reduction measures. Management and learning are structured in an inverted pyramid, from the health care centre to the Ministry of Health, with phases of detection, reporting, classification, analysis, implementation of improvements, and feedback.6
Despite national reports, analysis at the regional level can offer a more granular and useful perspective. This study seeks to contribute to improving health care quality and reducing preventable risks in Aragon.
The objectives of this study were: 1) to analyse the frequency and distribution of reported incidents and adverse events based on notifier profile, area of occurrence, category, and risk level; 2) to identify conditioning factors (drivers) and actions taken; and 3) to propose improvement and action measures based on the information provided.
MethodStudy designDescriptive, cross-sectional prevalence study.
Setting and populationAragon, located in northeastern Spain, is an autonomous region of 47,697 km2 with a population of nearly 1.5 million. Its capital, Zaragoza, concentrates most specialised health care services. The Spanish health system is predominantly tax-funded and is founded on the principles of universality, free access, equity, and fair financing.12
The study included all 959 notifications (i.e., the entire dataset available during the study period, with no sampling performed) submitted to SiNASP in the 8 health areas of Aragon, Spain, during 2023. Aragon's public health care infrastructure includes 22 hospitals with 4124 beds and 13,046 reporting professionals; 14 of these hospitals were registered in SiNASP as of 31 December 2023.13–16
Data sourceData was provided by the Spanish Ministry of Health, with the corresponding authorisation from the Department of Health of the Government of Aragon. The dataset was presented in spreadsheet format and used for data organisation and statistical analysis.
Variables studiedThe study included all variables routinely collected by SiNASP, which are standardised within the reporting system. No additional selection or reclassification of variables was performed.
These include: area of occurrence (multiple-choice); notifier profession (multiple-choice); incident description (free text); incident category (multiple-choice); frequency/recurrence probability (very rare, infrequent, occasional, probable, or frequent); incident classification/type of harm (potential risk, incident not reaching patient, or incident reaching patient); patient age and sex; severity assessment code (SAC), automatically calculated based on incident severity and frequency; contributing factors (free text and multiple-choice); risk reduction measures (free text); and management actions (multiple-choice; e.g. notification to management, simplified root cause analysis, risk reduction mechanism, and follow-up).
SAC risk levels cannot be modified manually. Incidents with no patient harm or not reaching the patient are classified as “no SACS”.
Statistical analysisMicrosoft Office Excel gathered all data in spreadsheet format and was used for analysis. Data is analysed using descriptive statistics, with statistical methods including absolute numbers, percentages, measures of central tendency and dispersion, contingency tables, and graphical representations using bar and pie charts.
Free text analysisFree text fields were manually reviewed and analysed using qualitative descriptive analysis. Relevant incidents were identified through iterative reading and grouped into inductively generated thematic categories. Given the unstructured nature of the data, no automated coding or standardised classification was applied.
Ethical considerationsThe study adhered to ethical regulations, ensuring confidentiality and anonymisation of data to protect patients, professionals, and centres. Authorisation was obtained from the Ethics Committee for Research of the Autonomous Community of Aragon (CEICA) (Authorisation C.I. PI24/546, Act No. 23/2024, December 18, 2024). No hospital-specific data or identifiable notifier information was used.
ResultsA total of 959 notifications were analysed following the main variables collected by the SiNASP.
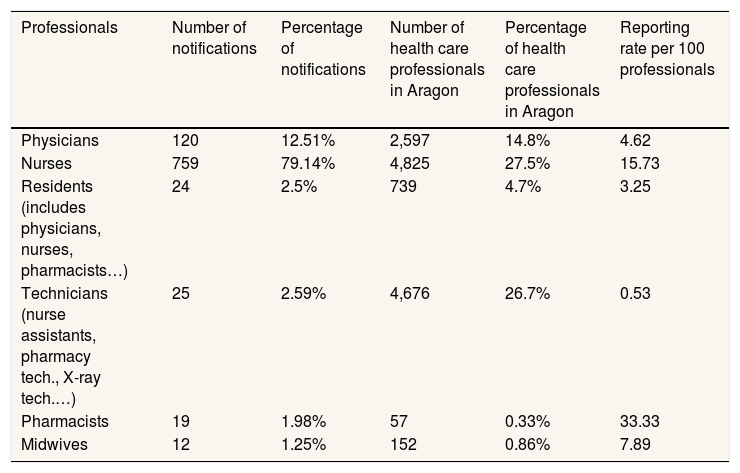
Notifier professionNurses accounted for the largest proportion (79.14%) of notifications, followed by physicians (12.51%), residents (2.5%), nursing assistant (2.29%), pharmacists (1.98%), and midwives (1.25%). There was a noticeable disparity between notification rates and staff proportions: pharmacists had the highest notification rate per 100 professionals (33.33), followed by nurses (15.73) and midwives (7.89) (Table 1).
Reporting professionals in Aragon's health care system during 2023.16
| Professionals | Number of notifications | Percentage of notifications | Number of health care professionals in Aragon | Percentage of health care professionals in Aragon | Reporting rate per 100 professionals |
|---|---|---|---|---|---|
| Physicians | 120 | 12.51% | 2,597 | 14.8% | 4.62 |
| Nurses | 759 | 79.14% | 4,825 | 27.5% | 15.73 |
| Residents (includes physicians, nurses, pharmacists…) | 24 | 2.5% | 739 | 4.7% | 3.25 |
| Technicians (nurse assistants, pharmacy tech., X-ray tech.…) | 25 | 2.59% | 4,676 | 26.7% | 0.53 |
| Pharmacists | 19 | 1.98% | 57 | 0.33% | 33.33 |
| Midwives | 12 | 1.25% | 152 | 0.86% | 7.89 |
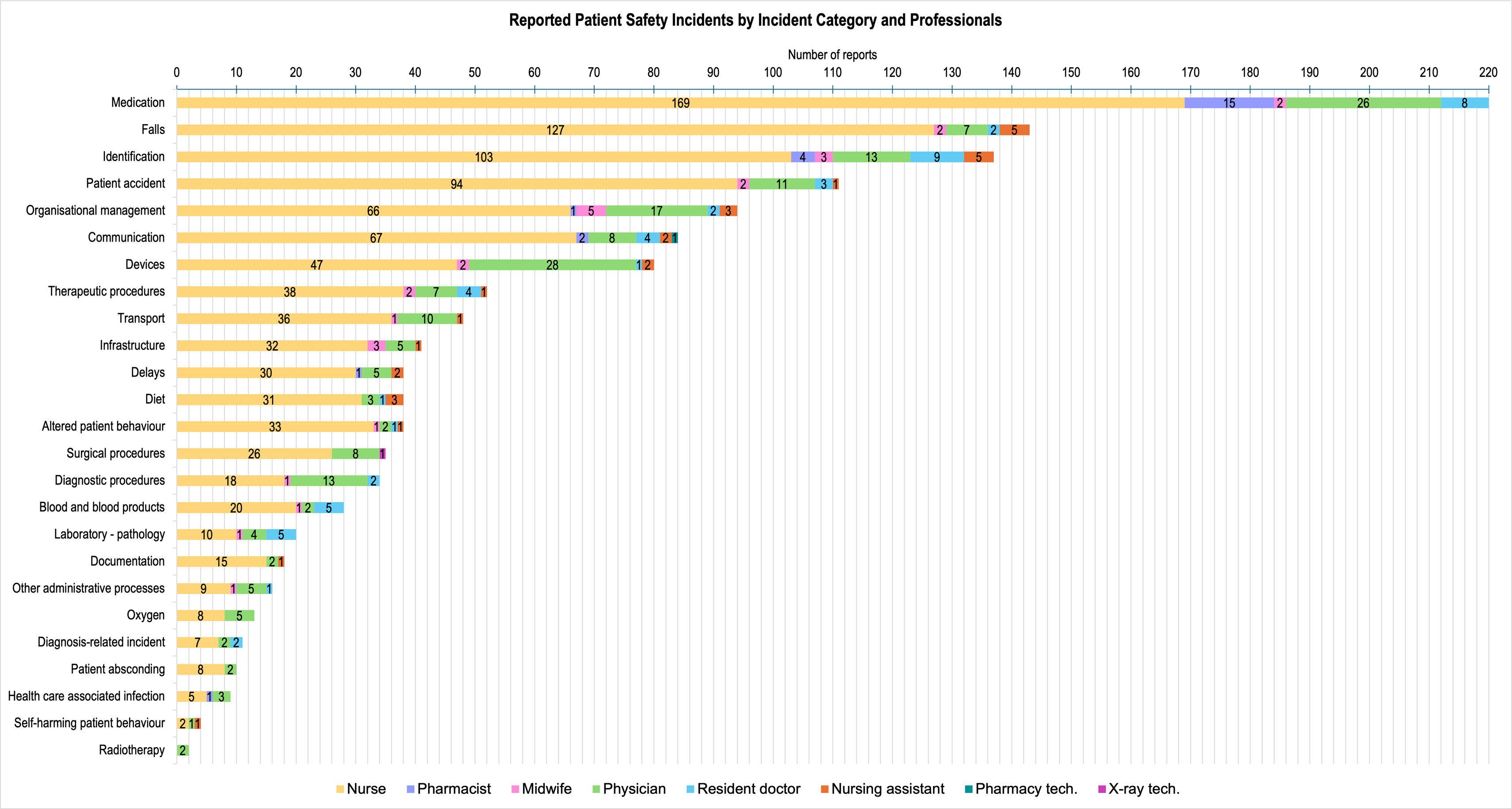
Medication-related incidents were the most frequent (22.9%), followed by falls (14.9%) and identification issues (6.2%) (Fig. 1).

Of all falls, a total of 67.1% were medication-related, with sedatives/hypnotics implicated in 50% of these cases. Anticoagulants, antihypertensives, and diuretics were also frequently involved.
There were differences in the types of incidents reported by each professional group (Fig. 1). Inside the category of medication-related incidents (n=220), the nursing staff reported, by far, the most incidents (169; 76.82%), followed by physicians (26; 11.82%) and pharmacists (15; 6.82%). Inside the category of falls (n=143), the nursing staff also leaded in reports (127; 88.81%). Similarly, the category of identification errors (n=137) was predominantly reported by nurses (103; 75.18%).
SAC levelsNearly half of the incidents (44.53%) were classified as “no SACS”, indicating no risk or unclassifiable harm. Low-risk incidents (SAC4) predominated (31.28%), with percentages decreasing for higher severity (SAC3, 17%; SAC2, 6.88%; SAC1, 0.31%).
Nurses were the only group to report SAC1 incidents (0.74% of their notifications). Pharmacists reported the highest proportion of higher-risk incidents (SAC2) compared to other groups (25% of their notifications).
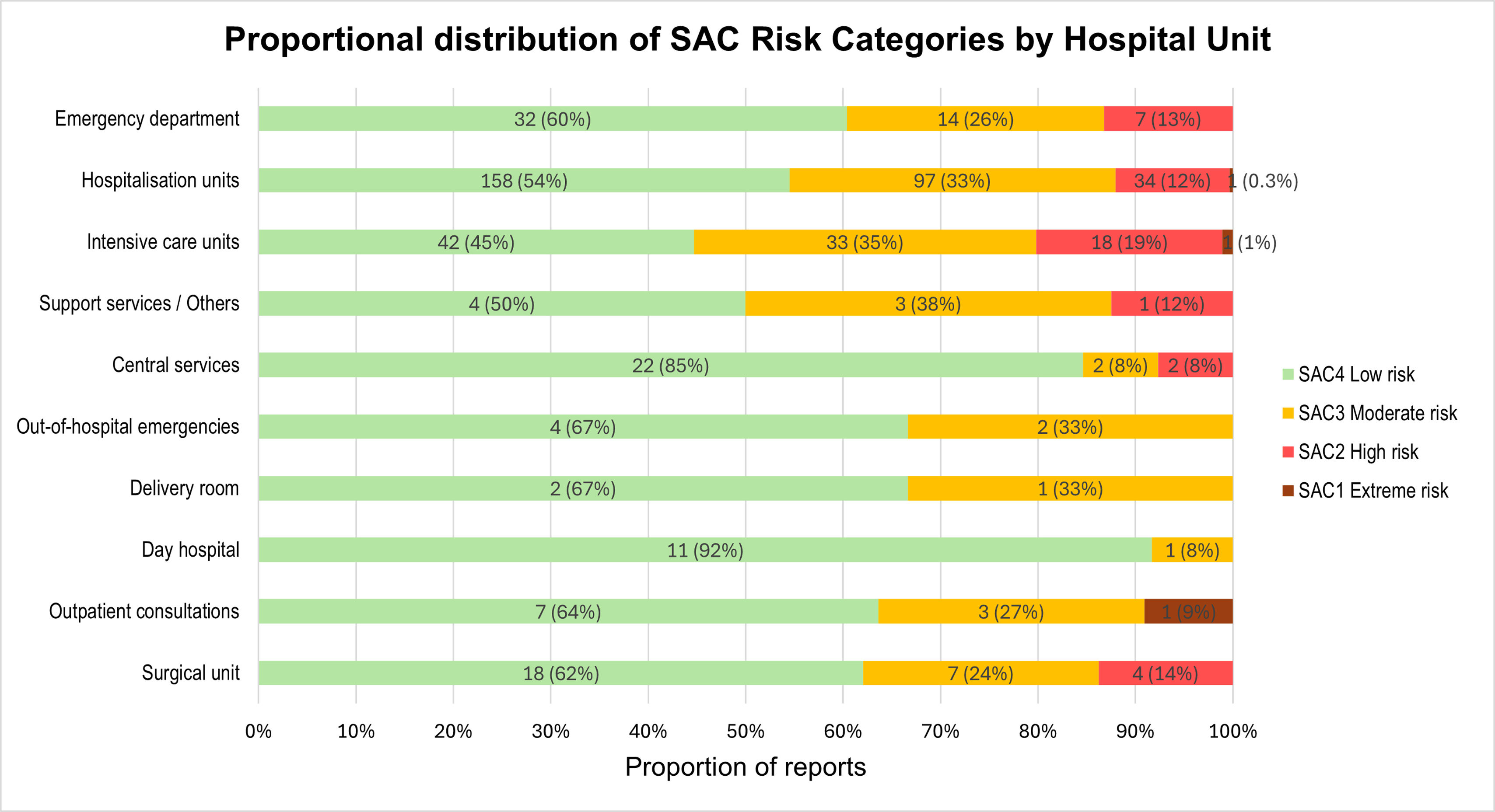
Globally, low-risk incidents (SAC4) were predominant in most areas (Fig. 2). Although low risk predominated, areas such as intensive care units and central services showed a significant presence of high-risk incidents (SAC2).
Area of occurrence and patient type
Of all reports taking place in hospitalisation units (n=497) concentrated most of the reports from nurses (423; 85.11%), residents (15; 3.02%), and pharmacists (14; 2.82%). The intensive care unit (ICU) (n=135) was the area in which most of physicians’ incidents took place (25.83% out of all physician reports).
Regarding areas of occurrence, day hospitals accounted for the largest proportion of reports (51.82%), followed by outpatient clinics (14.08%), the emergency department (9.7%), and the operating theatre (8.76%).
Of total reports, 139 (14.49%) involved paediatric patients. Of these, 58 (41.73% of paediatric reports and 6.04% of the total) concerned neonates, and 49 (35.25% of paediatric reports and 5.11% of the total) concerned the paediatric ICU.
Time of notification47.3% of all notifications occurred outside regular working hours (8:00-15:00h). A total of 16.37% were on weekends or holidays.
Recurring issuesRecurring issues included medication errors (prescription, administration, preparation), patient falls (lack of supervision, equipment), patient identification errors (labels, names, documentation), communication problems (unclear orders, handover, critical values), equipment/material issues (malfunctions, lack of availability), staffing/workload problems (lack of personnel, high workload in night shifts/weekends), lack of staff continuity (e.g. in Paediatric ICU), lack of digitalisation (manual records in OR/ICU), ambulance service issues (strikes, delays, resource allocation), non-compliance with protocols.
Highlighted severe incidentsHighlighted severe incidents included patient falling off the operating table (no major consequences), incorrect biopsy sample preservation (requiring repetition), unnecessary radiation exposure, incorrect parenteral nutrition dose, patient suffocation with a trash bag, propofol overdose with critical outcomes, and haemodialysis equipment malfunction causing severe hypotension.
Contributing factorsContributing factors (reported by 928 notifiers), categorising them as per the source, included personnel factors (poor communication, staffing, training, fatigue), patient-related factors (disorientation, mobility, identification issues), medication-related factors (dosing, similar appearance), non-compliance with protocols, defective material, and infrastructure issues (visibility, temperature, maintenance).
Risk reduction measuresRisk reduction measures (proposed by 922 notifiers) included thorough patient identification, correct medication administration (double-checks, computerisation, proper labelling), allergy management, fall prevention (bed rails, risk scales), improved communication (inter-professional, patient/family), adequate staffing and qualified personnel (stable contracts, specific training), and improved hospital furniture/facilities (maintenance, IT systems).
DiscussionCompared with other studies, the high notification rate among nurses aligns with their prolonged patient contact, higher numbers, and strong safety culture of this professional group. On the same line, higher proportion of high risk (SAC2) adverse events reported by pharmacists is consistent with national literature, reflecting their critical role in medication safety.15
A significant number of notifications occur outside regular working hours (47.3%) and on weekends, possibly indicating time constraints for professionals to notify incidents.
Specific areas like ICU and paediatric units show higher notification rates, potentially due to a more established proactive safety culture.
The study's findings, consistent with much of the international literature, highlight systemic failures (logistics, staffing levels, workload, infrastructure, IT systems) as major drivers of incidents, rather than solely individual human error. Likewise, the findings of this study appear broadly consistent with national SiNASP reports, which describe similar patterns in incident typology, notifier profile, and contributing factors. Recent national reports highlight the predominance of medication-related incidents, communication failures, and organisational factors as frequent contributors to adverse events, supporting the systemic nature of patient safety risks observed in our regional data. Although direct comparisons must be interpreted cautiously due to methodological and contextual differences, these similarities suggest that the patterns identified in Aragon may reflect broader trends within the Spanish National Health System.15
Nevertheless, external validity should be interpreted considering regional organisational structures, safety culture maturity, and implementation strategies of incident reporting systems. Variability in reporting behaviour, professional engagement, and local safety initiatives may influence notification patterns across regions. Therefore, while results provide relevant insights aligned with national evidence, they should be interpreted as complementary to broader surveillance and learning initiatives rather than fully generalisable estimates of incident frequency or severity.
The findings of the study have several implications at different levels of the healthcare system.
From a policy and regulatory perspective, strengthening legal and organisational frameworks that protect notifiers remains a priority. Learning from international experiences, promoting a non-punitive reporting environment may facilitate participation and improve the quality of information collected. Additionally, policies encouraging patient and family involvement in reporting could contribute to identifying risks not always captured by healthcare professionals.
A “just culture” (balancing learning from errors with disciplinary actions) as advocated by the WHO is critically important. Spain's SiNASP lacks specific legal protections for notifiers and “second victims”, contrasting this with models in Denmark and Italy that provide such safeguards to encourage reporting and learning. This absence likely contributes to the underreporting of severe events. It's relevant to connect the vulnerability of professionals involved in adverse events to the concept of “second victims”, highlighting the need for support systems.17–19
At the organisational level, hospital management and intermediate leadership play a key role in transforming reporting into effective learning and improvement strategies. This includes allocating resources to address structural drivers, strengthening communication protocols, improving patient identification procedures, enhancing medication management systems, and ensuring adequate infrastructure maintenance. Intermediate managers are particularly important in promoting local safety culture, facilitating feedback to professionals, and supporting the implementation of corrective actions derived from incident analysis.
From the perspective of healthcare professionals, integrating patient safety training into undergraduate education and continuing professional development may reinforce engagement with reporting systems such as SiNASP, with practical strategies to promote reporting such as including structured self-assessment following clinical activity.
Strengths and limitationsThis study provides a detailed regional analysis of patient safety incidents using a national reporting system (SiNASP), offering valuable insights into local challenges and contributing factors. The qualitative data from free text descriptions improves the understanding of incident dynamics and proposed solutions. Ethical considerations, including anonymisation and CEICA approval, ensure data integrity and confidentiality.
However, several limitations must be recognized. First, the voluntary and anonymous nature of the reporting system constitutes a major limitation, as it leads to underreporting of incidents and may limit the representativeness of the recorded data in relation to the actual frequency and nature of adverse events. Fear of reprisal for severe events, omission of mild or repetitive incidents, and retrospective distortion bias (events appearing more preventable in hindsight) may further influence reporting patterns.
In addition, SiNASP explicitly excludes certain incidents involving severe harm with potential legal implications. Therefore, beyond underreporting, the system may present limitations in terms of completeness, particularly regarding high-severity events, which must be considered when interpreting the results.
Another relevant limitation relates to the interpretation of contributing factors and improvement actions proposed by the notifier, particularly in free text fields. These variables depend on the individual notifier's experience, analytical capacity and perception of the incident. Incident reporting systems may occasionally be used as a channel to express organisational concerns or professional dissatisfaction, which can influence the content and validity of the reported information.
Furthermore, anonymity limits the possibility of verifying reported data, which may lead to incomplete or inconsistent descriptions. This limitation interacts with known barriers to reporting, including variability in patient safety culture, limited perception of system usefulness, fear of repercussions, insufficient training, and time constraints.
Finally, restricting the study period to one year provides a cross-sectional snapshot and does not allow assessment of temporal trends. Longitudinal analyses would be required to explore reporting patterns over time and to evaluate the evolution of SiNASP as a valuable patient safety tool among healthcare professionals.
ConclusionsThe most frequently reported incidents to SiNASP in Aragon (Spain) in 2023 were related to medication (22.9%), falls (14.9%), and identification errors (6.2%). Incidents without harm (44.53%) or with low risk (SAC4; 31.28%) predominated. Most reports originated from nursing staff (79.14%), and inpatient wards and ICU, particularly neonatology, were the settings with the highest reporting frequency. These findings highlight the multifactorial nature and pervasiveness of patient safety issues in healthcare.
The main contributing factors identified included deficiencies in staffing (qualification, workforce levels), patient frailty, lack of protocol implementation, medical and care errors related to medication, defective equipment and healthcare facilities, communication failures, and identification problems.
Proposed improvement measures focus on the implementation of double-checks and checklists, strengthening communication and healthcare staff training, fall prevention, and proper maintenance of hospital equipment and facilities. To optimise the reporting system, it is essential to reinforce professional training, introduce regulatory changes that protect reporters, and provide sufficient time to complete the process.
Availability of databases and material for replicationThe data that support the findings of this study were provided by the Spanish Ministry of Health, with the corresponding authorisation from the Department of Health of the Government of Aragon, under a confidentiality agreement. Restrictions apply to the availability of these data and the authors are not authorised to share or distribute these datasets. Interested researchers must apply for access directly through the Ministry of Health's official channels.
Incident reporting systems are a cornerstone of patient safety strategies worldwide, yet evidence on how they operate in real-world clinical settings, particularly across Europe, remains scarce.
What does this study add to the literature?This analysis of one year of hospital reports from Aragon (Spain) reveals key patterns in medication, falls and identification incidents, exposing weaknesses in communication and workforce stability.
What are the implications of the results?This study shows how national data can be translated into actionable learning, highlighting the value of robust reporting cultures to shape safer care, inform training priorities and guide policy development.
Rocío Zurriaga-Carda.
Transparency declarationThe corresponding author, on behalf of the other authors guarantee the accuracy, transparency and honesty of the data and information contained in the study, that no relevant information has been omitted and that all discrepancies between authors have been adequately resolved and described.
Authorship contributionsM. Doweidar: data analysis, interpretation, and drafting of the manuscript. C. Aibar-Remón: data interpretation, supervision, and review.
To the Subdirección General de Calidad Asistencial of the Dirección General de Salud Pública y Equidad en Salud del Ministerio de Sanidad for facilitating the data. To all professionals who made notifications to SiNASP in Aragon.











