






To estimate the prevalence of mpox vaccine uptake and its associated factors among gay, bisexual, and other men who have sex with men (GBMSM) in Spain, and to examine, among those who were not vaccinated, their intention to receive the vaccine and the factors linked to that intention.
MethodWe conducted a cross-sectional study using data from the Spanish subsample of the LIBERO-POX study (October 2022–March 2023), an online survey of adult people identifying as GBMSM in 10 Ibero-American countries participating in LIBERO-POX. We estimated mpox vaccine uptake and likelihood of vaccination among the unvaccinated, and analysed sociodemographic, psychosocial, and behavioural factors using Poisson regression with robust variance.
ResultsAmong 548 participants, 38.0% reported mpox vaccination. Of 338 unvaccinated individuals, 91.7% expressed high likelihood to vaccinate. Uptake was associated with being aged 30–49, living in larger municipalities, receiving information from health professionals, PrEP use, HIV status, and having more than 10 sexual partners in the last 6 months. High likelihood was instead linked to psychosocial perceptions, such as concern about mpox and perceived severity.
ConclusionsA gap exists between vaccination intention and uptake among GBMSM in Spain. Bridging this gap requires public health strategies that combine trusted, non-stigmatizing communication with measures addressing barriers to access (territorial disparities, limited sexual health services, and stigma), to achieve equitable vaccine coverage.
Estimar la prevalencia de la vacunación contra mpox y sus factores asociados en hombres gais, bisexuales y otros hombres que tienen relaciones sexuales con hombres (GBHSH) en España, y examinar, entre los que no se vacunaron, su intención de recibir la vacuna y los factores relacionados con esa intención.
MétodoEstudio transversal utilizando datos de la submuestra española del estudio LIBERO-POX (octubre de 2022 a marzo de 2023), que recopiló respuestas a una encuesta en línea realizada a personas mayores de edad, que se identificaban como GBHSH y que residían en los 10 países iberoamericanos participantes en el estudio LIBEROPOX. Se estimó la prevalencia de la aceptación de la vacuna contra mpox y la probabilidad de vacunarse entre las personas no vacunadas, y se analizaron los factores sociodemográficos asociados.
ResultadosDe los 548 participantes GBHSH, el 38,0% afirmaron haber recibido la vacuna contra mpox. De las 338 personas no vacunadas, el 91,7% expresaron una alta probabilidad de vacunarse. La vacunación se asoció significativamente con factores sociodemográficos y conductuales, como tener entre 30 y 49 años, vivir en municipios más grandes, recibir información de profesionales de la salud, usar PrEP, vivir con el VIH y tener más de 10 parejas sexuales en los últimos 6 meses. La alta probabilidad de vacunarse se asoció principalmente con percepciones psicosociales, como la preocupación por el mpox y la gravedad percibida de la infección.
ConclusionesExiste una clara brecha entre la intención de vacunarse y la aceptación real entre los GBHSH en España. Para reducir esta brecha se necesitan estrategias de salud pública que no solo proporcionen y promuevan información y motivación a través de mensajes fiables y no estigmatizantes, sino que también aborden las barreras de acceso (como las desigualdades territoriales, el acceso limitado a los servicios de salud sexual y el estigma) para garantizar una cobertura vacunal equitativa y eficaz.
The monkeypox virus (MPXV) causes a zoonotic disease (mpox) endemic to several African countries.1 By July 2022, the World Health Organization (WHO) declared it a public health emergency of international concern.2 In Spain, a total of 7,521 new cases were reported in 2022 and 325 additional cases in 2023, making Spain one of the most affected countries in the European Union.3
Although MPXV clade IIb is self-limited, a small proportion of cases require hospitalization (7%), with a case fatality rate of 0.1%.4 The clade IIb MPXV outbreak primarily spread through close physical contact (which often takes place during sexual encounters but is not strictly limited to sexual transmission), with most cases involving men, particularly gay, bisexual, and other men who have sex with men (GBMSM), aged 30-50 years.4–6 In response to the rapid rise in cases, swift actions were taken, including surveillance, contact tracing, and vaccination of high-risk groups.2,7 In Spain, vaccination began in June 2022, although initial vaccine availability was limited.8 As a result, individuals engaging in high-risk sexual behaviours —such as having multiple partners or participating in group sex— were prioritized for pre-exposure prophylaxis, particularly GBMSM, along with those with occupational exposure risks and individuals living with HIV or on PrEP.8
Vaccination played a key role in controlling the outbreak, together with the reduction in the susceptible population following a high number of infections and behavioural changes among higher-risk groups, partly driven by risk communication efforts.9 Nevertheless, vaccine uptake varied globally due to differences in availability, accessibility, and national policies.10 A meta-analysis found that global vaccine uptake stood at only and 30.9%, with Europe having the highest rate at 33.5%.10 Within Europe, a study conducted in the United Kingdom observed a significantly higher uptake of 69%.11 In the case of Spain, although there are no specific studies quantifying the percentage of vaccinated individuals, available data indicate that, by December 2022, over 25,000 vaccine doses had been administered, including both partial and complete doses.12
To date, no data are available regarding mpox vaccine uptake, intention, and the associated factors during the 2022-2023 outbreak within the Spanish context. This underscores the importance of identifying the factors associated with mpox vaccine uptake and intention in a context of vaccine availability, to inform strategies aimed at increasing vaccination coverage. The Health Belief Model provides a theoretical framework to understand preventive health behaviours, including vaccination, by positing that individuals’ actions are influenced by a combination of background or modifying factors, health-related beliefs, and cues to action.13 First, modifying factors, including sociodemographic characteristics, health-related behaviours, and psychosocial factors, shape individuals’ beliefs about a health threat. Second, health-related beliefs, such as perceived susceptibility, perceived severity, and perceived benefits and barriers to action, determine motivation to engage in preventive behaviours. Third, cues to action represent external or situational triggers that can activate the decision to adopt a preventive behaviour. Together, these components offer a structured approach to examining how individual, social, and contextual factors interact to influence health-related decision-making. Complementarily, access-oriented frameworks such as Tanahashi's model emphasise that effective health services coverage (such as vaccination) depends not only on individual motivation and availability, but also on the acceptability of services, which may be shaped by broader psychosocial and social barriers.14
In the context of mpox, relevant modifying factors include sociodemographic characteristics, health-related factors such as HIV status or PrEP use, and psychosocial factors including perceived stigma, which can act as a barrier to access health services due to fear of social judgment.10 Health-related beliefs encompass worry about mpox, perceived susceptibility to infection, and perceived severity of the disease, which together shape individuals’ motivation to vaccinate. Finally, cues to action include sexual behaviours that may increase perceived exposure risk, as well as receiving mpox-related information from healthcare professionals, both of which can trigger preventive actions such as vaccination.15,16
Therefore, this study pursues two objectives: 1) to estimate the prevalence of mpox vaccine uptake and its associated factors among GBMSM in Spain; and 2) to examine, among those who were not vaccinated, their intention to receive the vaccine and the factors linked to that intention.
MethodStudy designCross-sectional study with data from the LIBERO-POX project, an international study coordinated by the Right PLUS network (a network of both academic and community-based organisation from Latin America, Spain and Portugal, coordinated from Coalition PLUS, https://www.coalitionplus.org/rightplus/), which assessed knowledge, attitudes, and behaviours related to mpox among GBMSM in 10 countries: Argentina, Brazil, Bolivia, Chile, Colombia, Ecuador, Spain, Guatemala, Peru and Portugal. Data were collected from October 2022 to March 2023.
Recruitment and study populationA convenience sample was recruited using multiple online strategies, including advertisements and direct outreach through dating applications, websites, and social media platforms, as well as the dissemination of survey links via banners and instant messages. In addition, community-based organizations and peer workers shared the survey with individuals who had previously consented to being contacted. During the recruitment period, repeated reminders were distributed through the same channels and supplemented with additional dissemination strategies to maximize reach and response. Eligibility for the LIBEROPOX project was assessed on the survey landing page, which included detailed study information and an electronic informed consent form (the participant information sheet and informed consent form can be found in Supplementary Material 1). Individuals aged 18 years or older, residing in one of the participating countries, and self-identifying as men who have sex with men were eligible to participate. The questionnaire link hosted on LimeSurvey was accessed 26,909 times. Of these accesses, 9446 resulted in dropouts without any information provided, while 17,463 included a response to the country-of-birth question. Among these respondents, 1178 answered that they lived in Spain, which was our study population for this analysis. Of these remaining accesses, 1,155 participants provided consent to proceed with the questionnaire, and 627 ultimately completed and submitted it (54.3% of those who provided consent; see Supplementary Figure 1 for the participant flow diagram). Measures were implemented to ensure data quality and to verify that responses were unique, thereby reducing the risk of automated or malicious submissions.
Data collection toolThe study questionnaire was an open survey, and it was developed based on previously used instruments assessing mpox-related behaviours and perceptions among GBMSM populations in Europe,17,18 which were adapted for the LIBERO-POX project (the study questionnaire can be found in Supplementary Material 2). The questionnaire was translated and culturally adapted into Spanish, European Portuguese, and Brazilian Portuguese, and tested before data collection. It covered a broad range of domains, including sociodemographic characteristics, HIV status and PrEP use, psychosocial factors, sexual and substance use behaviours, behavioural changes in response to the mpox outbreak, mpox diagnosis and exposure within social networks, preventive practices and intentions, acceptability of mpox testing and vaccination, perceptions and attitudes toward mpox, sources of information, and mpox-related knowledge.
Study sampleThe present analysis used only data from Spain. Data from 627 GBMSM over 18 years old who lived in Spain were collected (7% of the total sample of the LIBERO-POX project). Those subjects who had missing values in several variables were excluded (n=18). Moreover, participants with a previous mpox diagnosis were excluded from the analysis because we could not determine the date of diagnosis and therefore could not assess whether they were eligible to receive the vaccine or not (n=53).
Dependent variables- 1)
Mpox vaccination uptake
Vaccination uptake was determined by asking the following question: “Have you ever received the monkeypox vaccine?” with three possible answers (Yes/No/I prefer not to answer). People who did not want to answer were excluded (n=8), leaving a final sample of 548 people for the first study objective (uptake population).
- 2)
Likelihood to receive the mpox vaccine
Likelihood to receive the mpox vaccine was measured by asking participants who were not previously vaccinated (n=340) the following question: “If you were offered a smallpox vaccine to prevent the severe form of monkeypox, how likely would you be to take it?”, with five possible answers from “Not likely” to “Extremely likely”. Those who indicated they were “Not at all likely” or “Not very likely” were categorized as having low likelihood to be vaccinated, while those who responded, “Moderately likely,” “Very likely,” or “Extremely likely” were grouped as having high likelihood to be vaccinated. People who did not want to answer were excluded (n=2), leaving a final sample of 338 people for the second study objective (likelihood population).
Independent variables- 1)
Modifying factors
Three types of modifying factors were included:
- •
Sociodemographic variables: age, highest degree of education, employment, country of birth, municipality size.
- •
Health related variables: having access to the public health care system or private health insurance, HIV status and being on PrEP.
- •
Psychosocial variables: variables assessing perceived stigma toward the GBMSM community in the context of mpox were included. For example, participants were asked: “To what extent do you think monkeypox can be used to stigmatize gay men?”.
- 2)
Mpox-related beliefs
Participants were asked about their worry regarding mpox infection, their perceived risk of infection, and their perception of the severity of mpox infection.
- 3)
Cues to action
Having practiced chemsex in the last 6 months, number of sexual partners in the last 6 months, frequency of attending sex-on-premises venues (SOPV: e.g., saunas, dark rooms, private parties) in the last 6 months and having received information about mpox from a health care professional.
Statistical analysisA descriptive analysis was first conducted, followed by an analytical approach divided into two parts: first on the full sample, then on the unvaccinated subgroup. The first part analysed the entire sample to estimate mpox vaccination prevalence and identify associated factors. The second part focused on unvaccinated individuals, examining the prevalence of likelihood to receive the vaccine and associated factors. Prevalence estimates for both vaccination uptake and likelihood, along with 95% confidence intervals (95% CI), were stratified by independent variables. To identify factors linked to these outcomes, Poisson regression models with robust variance were used, providing prevalence ratios (PR) and 95% CI.19 Unadjusted models were first applied to explore associations, with significant variables (p<0.05) included in adjusted models. These models were refined through backward elimination, retaining only statistically significant variables (p <0.05). Given the imbalance in the outcome distribution in the unvaccinated subgroup, two sensitivity analyses were conducted: 1) penalized logistic regression using Firth's correction, both with and without adjustment for age, education, and employment status, and 2) non-parametric bootstrap confidence intervals (2000 replicates) for the unvaccinated Poisson regression models. Moreover, an additional descriptive analysis was conducted to compare the characteristics and mpox-related knowledge of unvaccinated individuals, stratified by their likelihood of receiving the mpox vaccine. All analyses were conducted using Stata 18.20
Ethical considerationsAll the participants signed an online informed consent form to participate in the study, prior to answering the survey. The questionnaire was voluntary and anonymous, since no data that would allow participants’ identification or tracking were requested. Participants could leave the study at any moment without saving their answers. No incentives were offered. The survey was designed, implemented, and reported in accordance with established recommendations for internet-based surveys, including the CHERRIES checklist, and it follows the principles of the Helsinki Declaration. The present study has been evaluated and approved by the Ethics Committee of the Hospital Germans Trias i Pujol, with the reference number PI-22-225.
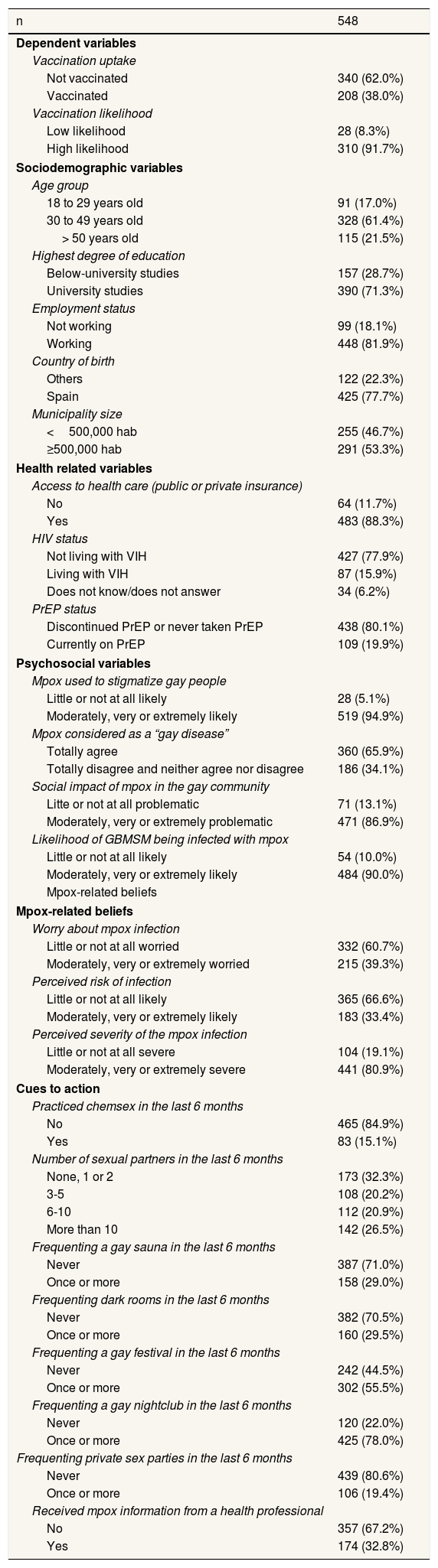
ResultsParticipant's characteristicsA total of 548 participants were included in the study. Table 1 summarizes the characteristics of the participants. Overall, 38.0% of participants had been vaccinated against mpox. Among the unvaccinated (n=338), 91.7% expressed high likelihood to receive the vaccine if offered.
Characteristics of the Spanish GBMSM sample analysed in our study.
| n | 548 |
|---|---|
| Dependent variables | |
| Vaccination uptake | |
| Not vaccinated | 340 (62.0%) |
| Vaccinated | 208 (38.0%) |
| Vaccination likelihood | |
| Low likelihood | 28 (8.3%) |
| High likelihood | 310 (91.7%) |
| Sociodemographic variables | |
| Age group | |
| 18 to 29 years old | 91 (17.0%) |
| 30 to 49 years old | 328 (61.4%) |
| > 50 years old | 115 (21.5%) |
| Highest degree of education | |
| Below-university studies | 157 (28.7%) |
| University studies | 390 (71.3%) |
| Employment status | |
| Not working | 99 (18.1%) |
| Working | 448 (81.9%) |
| Country of birth | |
| Others | 122 (22.3%) |
| Spain | 425 (77.7%) |
| Municipality size | |
| <500,000 hab | 255 (46.7%) |
| ≥500,000 hab | 291 (53.3%) |
| Health related variables | |
| Access to health care (public or private insurance) | |
| No | 64 (11.7%) |
| Yes | 483 (88.3%) |
| HIV status | |
| Not living with VIH | 427 (77.9%) |
| Living with VIH | 87 (15.9%) |
| Does not know/does not answer | 34 (6.2%) |
| PrEP status | |
| Discontinued PrEP or never taken PrEP | 438 (80.1%) |
| Currently on PrEP | 109 (19.9%) |
| Psychosocial variables | |
| Mpox used to stigmatize gay people | |
| Little or not at all likely | 28 (5.1%) |
| Moderately, very or extremely likely | 519 (94.9%) |
| Mpox considered as a “gay disease” | |
| Totally agree | 360 (65.9%) |
| Totally disagree and neither agree nor disagree | 186 (34.1%) |
| Social impact of mpox in the gay community | |
| Litte or not at all problematic | 71 (13.1%) |
| Moderately, very or extremely problematic | 471 (86.9%) |
| Likelihood of GBMSM being infected with mpox | |
| Little or not at all likely | 54 (10.0%) |
| Moderately, very or extremely likely | 484 (90.0%) |
| Mpox-related beliefs | |
| Mpox-related beliefs | |
| Worry about mpox infection | |
| Little or not at all worried | 332 (60.7%) |
| Moderately, very or extremely worried | 215 (39.3%) |
| Perceived risk of infection | |
| Little or not at all likely | 365 (66.6%) |
| Moderately, very or extremely likely | 183 (33.4%) |
| Perceived severity of the mpox infection | |
| Little or not at all severe | 104 (19.1%) |
| Moderately, very or extremely severe | 441 (80.9%) |
| Cues to action | |
| Practiced chemsex in the last 6 months | |
| No | 465 (84.9%) |
| Yes | 83 (15.1%) |
| Number of sexual partners in the last 6 months | |
| None, 1 or 2 | 173 (32.3%) |
| 3-5 | 108 (20.2%) |
| 6-10 | 112 (20.9%) |
| More than 10 | 142 (26.5%) |
| Frequenting a gay sauna in the last 6 months | |
| Never | 387 (71.0%) |
| Once or more | 158 (29.0%) |
| Frequenting dark rooms in the last 6 months | |
| Never | 382 (70.5%) |
| Once or more | 160 (29.5%) |
| Frequenting a gay festival in the last 6 months | |
| Never | 242 (44.5%) |
| Once or more | 302 (55.5%) |
| Frequenting a gay nightclub in the last 6 months | |
| Never | 120 (22.0%) |
| Once or more | 425 (78.0%) |
| Frequenting private sex parties in the last 6 months | |
| Never | 439 (80.6%) |
| Once or more | 106 (19.4%) |
| Received mpox information from a health professional | |
| No | 357 (67.2%) |
| Yes | 174 (32.8%) |
GBMSM: gay, bisexual, and other men who have sex with men; HIV: human immunodeficiency virus; PrEP: pre-exposure prophylaxis.
Most participants were aged 30-49 years (61.4%), had university-level education (71.3%), were employed (81.9%), and had access to healthcare (88.3%). In terms of psychosocial factors, 60.7% reported low or no concern about contracting mpox, and 66.6% perceived their risk as low. However, 80.9% rated the disease severity as moderate to high. A large majority (94.9%) believed that mpox was used to stigmatize the gay community, and 65.9% agreed that the general population was moderately, very or extremely likely to use mpox to stigmatise gay people.
Regarding sexual health and behaviours, 15.9% were living with HIV, 19.9% reported current PrEP use, and 15.1% had engaged in chemsex in the previous six months. Furthermore, 26.5% reported having had more than 10 sexual partners in the past 6 months.
Supplementary Table 1 presents the characteristics of the unvaccinated sample according to their likelihood to receive the mpox vaccine. Individuals with low likelihood to vaccinate reported lower concern about contracting mpox (p=0.002), lower perceived risk (p=0.045) and lower severity (p=0.002) of the mpox infection, compared to individuals with high likelihood. Moreover, they perceived mpox infection as little or not at all problematic in terms of social consequences (p=0.045).
Supplementary Table 2 presents mpox-related knowledge regarding transmission, symptoms, and preventive measures, stratified by individuals’ likelihood of receiving the mpox vaccine. Individuals with a low likelihood of vaccination more frequently reported either complete disagreement or neutral responses (neither agree nor disagree) to several statements, particularly those related to mpox transmission (e.g., transmission through direct contact, secretions, or lesions) and symptoms (e.g., variability in severity and symptom presentation). This pattern was especially pronounced for statements concerning preventive strategies. Specifically, individuals with a low likelihood of vaccination were more likely to disagree with measures such as limiting direct contact with diagnosed individuals, exchanging contact information with sexual partners, using condoms during oral sex, cleaning and disinfecting contaminated surfaces or clothing, and having been vaccinated (either against human smallpox during childhood or with a WHO-approved vaccine to prevent mpox).
Mpox vaccination uptake and associated factorsTable 2 shows the prevalence of vaccination uptake and unadjusted and adjusted PR. The global prevalence of vaccination uptake was 38.0%. GBMSM aged 30 to 49 years old reported higher vaccination than those older or younger (43.9%, 31.6%, and 26.4%, respectively). Moreover, individuals who lived in a bigger municipality and who had received mpox information from a health professional reported a higher vaccination uptake (46.7% vs. 28.3% and 64.2% vs. 26.9%, respectively). Those who practiced chemsex in the last 6 months were more vaccinated than those who did not (55.4% vs. 34.9%). Similarly, GBMSM who were on PrEP reported higher vaccination uptake that those who were not (78.0% vs. 28.1%).
Prevalence and 95% confidence interval, and unadjusted and adjusted prevalence ratios, of mpox vaccination uptake according to study variables.
| n | % (95%CI) | Unadjusted model | Adjusted modela | |||
|---|---|---|---|---|---|---|
| n (total) | 548 | PR | 95% CI | aPR | 95%CI | |
| Sociodemographic variables | ||||||
| Age group, years | ||||||
| 18-29 | 91 | 26.4 (18.3-36.4) | 1.00 | 1.00 | ||
| 30-49 | 328 | 43.9 (38.6-49.3) | 1.66 | (1.16-2.40) | 1.46 | (1.06-2.01) |
| > 50 | 114 | 31.6 (23.7-40.7) | 1.20 | (0.77-1.85) | 1.02 | (0.70-1.51) |
| Highest degree of education | ||||||
| Below-university studies | 155 | 32.3 (25.4 – 40.0) | 1.00 | |||
| University studies | 391 | 40.4 (35.6-45.4) | 1.25 | (0.97-1.62) | ||
| Employment status | ||||||
| Not working | 99 | 27.3 (19.4-36.9) | 1.00 | |||
| Working | 447 | 40.5 (36.0-45.1) | 1.48 | (1.06-2.09) | ||
| Country of birth | ||||||
| Others | 122 | 43.4 (34.9-52.4) | 1.00 | |||
| Spain | 424 | 36.6 (32.1-41.3) | 0.84 | (0.66-1.07) | ||
| Municipality size | ||||||
| <500,000 hab | 254 | 28.3 (23.1-34.2) | 1.00 | 1.00 | ||
| >500,000 hab | 291 | 46.7 (41.1-52.5) | 1.65 | (1.31-2.08) | 1.50 | (1.23-1.82) |
| Health related variables | ||||||
| Access to health care | ||||||
| No | 62 | 45.2 (33.3-57.6) | 1.00 | |||
| Yes | 484 | 37 (32.8-41.4) | 0.82 | (0.61-1.10) | ||
| HIV status | ||||||
| Not living with HIV | 426 | 39.2 (34.7-43.9) | 1.00 | 1.00 | ||
| Living with HIV | 87 | 41.4 (31.5-52) | 1.06 | (0.80-1.39) | 1.35 | (1.00-1.81) |
| Does not know/does not answer | 34 | 14.7 (6.2-30.9) | 0.38 | (0.17-0.85) | 0.53 | (0.21-1.31) |
| PrEP status | ||||||
| Discontinued PrEP or never taken PrEP | 437 | 28.1 (24.1-32.6) | 1.00 | 1.00 | ||
| Continuous PrEP | 109 | 78 (69.2-84.8) | 2.77 | (2.31-3.32) | 2.16 | (1.69-2.76) |
| Psychosocial variables | ||||||
| Mpox used to stigmatize gay people | ||||||
| Little or not at all likely | 28 | 46.4 (29.2-64.6) | 1.00 | |||
| Moderately, very or extremely likely | 518 | 37.6 (33.6-41.9) | 0.81 | (0.54-1.23) | ||
| Mpox considered as a “gay disease” | ||||||
| Totally agree | 359 | 41.2 (36.2-46.4) | 1.00 | |||
| Totally disagree and neither agree nor disagree | 186 | 32.3 (25.9-39.3) | 0.78 | (0.61-1.00) | ||
| Social impact of mpox in the gay community | ||||||
| Litte or not at all problematic | 72 | 48.6 (37.3-60.1) | 1.00 | |||
| Moderately, very or extremely problematic | 469 | 36.2 (32-40.7) | 0.75 | (0.57-0.97) | ||
| Likelihood of GBMSM being infected with mpox | ||||||
| Little or not at all likely | 54 | 35.2 (23.7-48.7) | 1.00 | |||
| Moderately, very or extremely likely | 483 | 38.5 (34.3-42.9) | 1.09 | (0.75-1.60) | ||
| Mpox-related beliefs | ||||||
| Worry about mpox infection | ||||||
| Little or not at all worried | 333 | 36 (31.0-41.3) | 1.00 | |||
| Moderately, very or extremely worried | 213 | 40.8 (34.4-47.6) | 1.13 | (0.91-1.41) | ||
| Perceived risk of infection | ||||||
| Little or not at all likely | 364 | 39.6 (34.7-44.7) | 1.00 | |||
| Moderately, very or extremely likely | 183 | 35 (28.4-42.2) | 0.88 | (0.70-1.12) | ||
| Perceived severity of the mpox infection | ||||||
| Little or not at all severe | 105 | 41 (32.0-50.6) | 1.00 | |||
| Moderately, very or extremely severe | 439 | 37.1 (32.7-41.8) | 0.91 | (0.70-1.18) | ||
| Cues to action | ||||||
| Practiced chemsex in the last 6 months | ||||||
| No | 464 | 34.9 (30.7-39.4) | 1.00 | |||
| Yes | 83 | 55.4 (44.6-65.7) | 1.59 | (1.26-2.00) | ||
| Number of sexual partners in the last 6 months | ||||||
| None, 1 or 2 | 172 | 18.6 (13.5-25.1) | 1.00 | 1.00 | ||
| 3-5 | 107 | 36.4 (27.9-46) | 1.96 | (1.31-2.92) | 1.71 | (1.17-2.52) |
| 6-10 | 113 | 43.4 (34.5-52.6) | 2.33 | (1.60-3.40) | 1.86 | (1.30-2.66) |
| More than 10 | 142 | 60.6 (52.3-68.3) | 3.26 | (2.32-4.57) | 1.74 | (1.22-2.50) |
| Frequenting a gay sauna in the last 6 months | ||||||
| Never | 387 | 33.3 (28.8-38.2) | 1.00 | |||
| Once or more | 157 | 50.3 (42.5-58.1) | 1.51 | (1.22-1.86) | ||
| Frequenting dark rooms in the last 6 months | ||||||
| Never | 381 | 34.1 (29.5-39) | 1.00 | |||
| Once or more | 160 | 47.5 (39.9-55.3) | 1.39 | (1.12-1.73) | ||
| Frequenting a gay festival in the last 6 months | ||||||
| Never | 241 | 28.2 (22.9-34.2) | 1.00 | |||
| Once or more | 302 | 46.4 (40.8-52) | 1.64 | (1.30-2.08) | ||
| Frequenting a gay nightclub in the last 6 months | ||||||
| Never | 119 | 21.8 (15.3-30.2) | 1.00 | 1.00 | ||
| Once or more | 425 | 42.6 (38-47.4) | 1.95 | (1.36-2.79) | 1.47 | (1.04-2.08) |
| Frequenting private sex parties in the last 6 months | ||||||
| Never | 438 | 34.7 (30.4-39.3) | 1.00 | |||
| Once or more | 106 | 51.9 (42.4-61.2) | 1.50 | (1.20-1.87) | ||
| Received mpox information from a health professional | ||||||
| No | 357 | 26.9 (22.5-31.7) | 1.00 | 1.00 | ||
| Yes | 173 | 64.2 (56.7- 71.0) | 2.39 | (1.95-2.93) | 1.62 | (1.32-1.98) |
aPR: adjusted prevalence ratio; 95%CI: 95% confidence interval; GBMSM: gay, bisexual, and other men who have sex with men; HIV: human immunodeficiency virus; PR: prevalence ratio; PrEP: pre-exposure prophylaxis.
The sociodemographic factors independently associated with vaccination uptake in the adjusted model were being 30-49 years old (aPR: 1.46; 95%CI: 1.06-2.01) and living in a big municipality (aPR: 1.50; 95%CI: 1.23-1.82). Having received information about mpox from a health professional was also associated with higher uptake (aPR: 1.62; 95%CI: 1.32-1.98). Regarding sexual health–related factors and behaviours, living with HIV (aPR: 1.35; 95%CI: 1.00-1.81), being on PrEP (aPR: 2.16; 95%CI: 1.69-2.76), having more than 2 sexual partners in the last 6 months (aPR: 1.71 for 3 to 5 partners, 1.86 for 6 to 10 partners, and 1.74 for more than 10 partners) and having attended a gay nightclub (aPR: 1.47; 95%CI: 1.04-2.08) were independently associated with higher vaccination uptake.
Likelihood to receive the mpox vaccine and associated factorsTable 3 presents the prevalence of high likelihood to receive mpox vaccine and unadjusted and adjusted PR. The prevalence of high likelihood to receive the mpox vaccine was 91.7% in non-vaccinated individuals. Participants who reported being moderately, very or extremely worried about contracting mpox, as well as those who perceived the infection as more severe, showed higher levels of vaccination likelihood compared to those with lower levels of concern and lower perceived severity (97.6% vs. 88.2%, and 93.8% vs. 82%, respectively).
Prevalence and 95% confidence interval, and unadjusted and adjusted prevalence ratios, of high likelihood to get vaccinated according to study variables.
| n | % (95%CI) | Unadjusted model | Adjusted modela | |||
|---|---|---|---|---|---|---|
| n (total) | 338 | PR | 95%CI | aRP | 95%CI | |
| Sociodemographic variables | ||||||
| Age group, years | ||||||
| 18-29 | 67 | 89.6 (79.6-95.0) | 1.00 | |||
| 30-49 | 183 | 91.3 (86.2-94.6) | 1.02 | (0.93-1.12) | ||
| > 50 | 78 | 93.6 (85.5-97.3) | 1.05 | (0.95-1.16) | ||
| Highest degree of education | ||||||
| Below-university studies | 105 | 94.3 (87.8-97.4) | 1.00 | |||
| University studies | 232 | 90.5 (86.0-93.7) | 0.96 | (0.90-1.02) | ||
| Employment status | ||||||
| Not working | 72 | 90.3 (80.9-95.3) | 1.00 | |||
| Working | 265 | 92.1 (88.1-94.8) | 1.02 | (0.94-1.11) | ||
| Country of birth | ||||||
| Others | 69 | 94.2 (85.5-97.8) | 1.00 | |||
| Spain | 268 | 91 (87.0-93.9) | 0.97 | (0.90-1.04) | ||
| Municipality size | ||||||
| <500,000 hab | 181 | 93.4 (88.7-96.2) | 1.00 | |||
| >500,000 hab | 155 | 89.7 (83.8-93.6) | 0.96 | (0.90-1.03) | ||
| Health related variables | ||||||
| Access to health care | ||||||
| No | 34 | 91.2 (75.9-97.1) | 1.00 | |||
| Yes | 304 | 91.8 (88.1-94.4) | 1.01 | (0.90-1.12) | ||
| HIV status | ||||||
| Not living with HIV | 258 | 91.1 (86.9-94.0) | 1.00 | |||
| Living with HIV | 51 | 94.1 (83.2-98.1) | 1.03 | (0.96-1.12) | ||
| Does not know/does not answer | 29 | 93.1 (76.2-98.3) | 1.02 | (0.92-1.14) | ||
| PrEP status | ||||||
| Discontinued PrEP or never taken PrEP | 313 | 91.7 (88.1-94.3) | 1.00 | |||
| Continuous PrEP | 24 | 91.7 (72.0-97.9) | 1.00 | (0.88-1.13) | ||
| Psychosocial variables | ||||||
| Mpox used to stigmatize gay people | ||||||
| Little or not at all likely | 15 | 93.3 (64.6-99.1) | 1.00 | |||
| Moderately, very or extremely likely | 322 | 91.9 (88.4-94.5) | 0.98 | (0.86-1.13) | ||
| Mpox considered as a “gay disease” | ||||||
| Totally agree | 211 | 92.9 (88.5-95.7) | 1.00 | |||
| Totally disagree and neither agree nor disagree | 125 | 90.4 (83.8-94.5) | 0.97 | (0.91-1.04) | ||
| Social impact of mpox in the gay community | ||||||
| Litte or not at all problematic | 36 | 83.3 (67.5-92.3) | 1.00 | |||
| Moderately, very or extremely problematic | 299 | 93 (89.5-95.4) | 1.12 | (0.96-1.30) | ||
| Likelihood of GBMSM being infected with mpox | ||||||
| Little or not at all likely | 35 | 88.6 (73.2-95.7) | 1.00 | |||
| Moderately, very or extremely likely | 296 | 91.9 (88.2-94.5) | 1.04 | (0.92-1.17) | ||
| Mpox-related beliefs | ||||||
| Worry about mpox infection | ||||||
| Little or not at all worried | 212 | 88.2 (83.1-91.9) | 1.00 | 1.00 | ||
| Moderately, very or extremely worried | 126 | 97.6 (92.9-99.2) | 1.11 | (1.05-1.17) | 1.08 | (1.02-1.14) |
| Perceived risk of infection | ||||||
| Little or not at all likely | 219 | 89.5 (84.7-92.9) | 1.00 | |||
| Moderately, very or extremely likely | 119 | 95.8 (90.3-98.2) | 1.07 | (1.01-1.14) | ||
| Perceived severity of the mpox infection | ||||||
| Little or not at all severe | 61 | 82 (70.2-89.7) | 1.00 | 1.00 | ||
| Moderately, very or extremely severe | 276 | 93.8 (90.3-96.1) | 1.14 | (1.01-1.29) | 1.13 | (1.00-1.28) |
| Cues to action | ||||||
| Practiced chemsex in the last 6 months | ||||||
| No | 301 | 91.7 (88.0-94.3) | 1.00 | |||
| Yes | 37 | 91.9 (77.6-97.4) | 1.00 | (0.91-1.11) | ||
| Number of sexual partners in the last 6 months | ||||||
| None, 1 or 2 | 140 | 87.9 (81.3-92.3) | 1.00 | 1.00 | ||
| 3-5 | 68 | 91.2 (81.7-96.0) | 1.04 | (0.94-1.14) | 1.03 | (0.94-1.13) |
| 6-10 | 63 | 95.2 (86.2-98.5) | 1.08 | (1.00-1.18) | 1.08 | (0.99-1.18) |
| More than 10 | 56 | 96.4 (86.8-99.1) | 1.10 | (1.01-1.19) | 1.09 | (1.01-1.17) |
| Frequenting a gay sauna in the last 6 months | ||||||
| Never | 257 | 91.1 (86.9-94.0) | 1.00 | |||
| Once or more | 78 | 93.6 (85.5-97.3) | 1.03 | (0.96-1.10) | ||
| Frequenting dark rooms in the last 6 months | ||||||
| Never | 250 | 91.6 (87.4-94.5) | 1.00 | |||
| Once or more | 84 | 91.7 (83.5-96.0) | 1.00 | (0.93-1.08) | ||
| Frequenting a gay festival in the last 6 months | ||||||
| Never | 172 | 93 (88.1-96.0) | 1.00 | |||
| Once or more | 162 | 90.1 (84.5-93.9) | 0.97 | (0.91-1.03) | ||
| Frequenting a gay nightclub in the last 6 months | ||||||
| Never | 92 | 94.6 (87.6-97.7) | 1.00 | |||
| Once or more | 244 | 90.6 (86.2-93.7) | 0.96 | (0.90-1.02) | ||
| Frequenting private sex parties in the last 6 months | ||||||
| Never | 285 | 91.2 (87.3-94.0) | 1.00 | |||
| Once or more | 51 | 94.1 (83.2-98.1) | 1.03 | (0.95-1.11) | ||
| Received mpox information from a health professional | ||||||
| No | 260 | 91.5 (87.5-94.4) | 1.00 | |||
| Yes | 62 | 91.9 (82.0-96.6) | 1.00 | (0.92-1.09) | ||
aPR: adjusted prevalence ratio; 95%CI: 95% confidence interval; GBMSM: gay, bisexual, and other men who have sex with men; HIV: human immunodeficiency virus; PR: prevalence ratio; PrEP: pre-exposure prophylaxis.
In the adjusted analysis only three factors remained independently associated with a higher likelihood to receive the mpox vaccine: being moderately, very or extremely worried about contracting mpox (aPR: 1.08; 95%CI: 1.02-1.14), perceiving the mpox infection as moderately, very or extremely severe (aPR: 1.13; 95%CI: 1.00-1.28) and having had more than 10 sexual partners in the last 6 months (aPR: 1.09; 95%CI: 1.01-1.17). Regarding the sensitivity analyses conducted, the results remained consistent across penalized logistic regression and bootstrap analyses (see Supplementary Tables 3 and 5). The inclusion of additional covariates (age, education, and employment status) did not materially alter the magnitude or direction of associations, supporting the robustness of the main findings (see Supplementary Tables 4 and 6).
DiscussionIn this study, 38% of GBMSM of our sample reported having received the mpox vaccine, while 91.7% of unvaccinated individuals expressed high likelihood to do so. The results suggest a gap between intention and uptake, with vaccination uptake mainly associated with sociodemographic and behavioural factors (such as age, urbanicity, PrEP use, and sexual activity) whereas vaccination likelihood was primarily linked to psychosocial variables, including concern about infection and perceived severity.
Young people (those under 30 years old) and older people (those aged>50 years old) were less likely to be vaccinated than those aged 30-49 years old. These findings are consistent with other studies, where young individuals reported less mpox vaccination uptake.11,15,21 Studies suggest that they could have less perception of severity and could be less linked to health services, which can be associated with lower access to mpox information and prevention measures, such as vaccination.21,22 Moreover, they can also experience more stigma, which also acts as a barrier to seek medical attention and diagnosis disclosure.23. For the older age group (>50 years), lower vaccination prevalence may be partly explained by the fact that they were not a prioritized group, as many individuals in this cohort received smallpox vaccination during childhood.
Participants residing in large municipalities (≥500,000 inhabitants) reported higher levels of vaccination uptake. This finding aligns with previous research24 and may be related to territorial disparities in access to healthcare. Less urbanized areas often lack specialized health services,25 which can limit the availability and accessibility of vaccination. Additionally, GBMSM living in rural or less urban settings may experience heightened levels of stigma, which has been described as a barrier to seeking care.26,27 In addition, the intradermal administration of the mpox vaccine in the forearm can leave visible marks,28 which have been described as stigmatising and associated with fears of being identified or judged.24
Use of PrEP, living with HIV and having more than 2 sexual partners in the last 6 months were also associated with higher vaccination uptake, in line with findings from previous studies.10,11,15,29 This association is consistent with vaccination strategies that prioritized individuals at elevated risk, such as people with multiple sexual partners, those who were on PrEP and people living with HIV.12 Furthermore, having attended a gay nightclub one or more times in the last six months was also associated with higher vaccination uptake. This finding may also reflect public health strategies that prioritized vaccination for individuals engaging in higher-risk practices,12 such as attending SOPV. In addition, information campaigns conducted in nightclubs (for example, through posters or outreach activities led by community-based organisations) may have further contributed to this association. Also, based on previous literature, attending SOPV has been associated with increased risk perception, which has in turn been associated with higher motivation.29
However, in our study, beliefs related to mpox were not significantly associated with actual vaccination uptake. Interestingly, beliefs were significantly related to the intention to get vaccinated. One possible explanation could be that perceived severity and concern about mpox are associated with individuals’ motivation and intention, but not necessarily linked with preventive actions. This finding may reflect the well-established gap between intention and behaviour, as described in health behaviour theories such as the theory of planned behaviour.30 While intentions are largely shaped by individual beliefs and perceptions, actual behaviour is also conditioned by the subjective norms within the community —specifically, the perceived social acceptance and support for vaccination among GBMSM. Social normalization of the vaccine can be a decisive factor in increasing intention; however, this motivation often remains latent when faced with external and structural factors, including access to services, logistical obstacles, or fear of stigma.
Specifically, our findings regarding healthcare provider advice illustrate this complexity. Such advice may be insufficient to bridge the intention-behavior gap unless supported by public health campaigns that promote visibility, legitimize the process, and reinforce the vaccine's importance within the community. Moreover, the influence of professional recommendations is contingent on a consistent link with the health system. For marginalized individuals, the absence of this connection means that verbal advice alone cannot overcome logistical barriers or systemic mistrust. To be effective, clinical recommendations must be paired with direct, low-barrier access and communication strategies that strengthen the social normalization of vaccination among GBMSM. This phenomenon is not unique to mpox. Previous studies in the context of the vaccination against the COVID-19 have shown that even highly motivated individuals may not act on their intentions when faced with such barriers.31 In the case of mpox, sociodemographic factors, such as socioeconomic status and education level, significantly influence mpox vaccination access, with higher education and income associated with increased uptake.10,11 Moreover, contextual factors, including territorial inequalities and perceived stigma, further hinder access, widening the gap between vaccination intention and actual uptake.26,27
A subgroup of particular relevance in our study comprises unvaccinated individuals who reported a low likelihood of receiving the mpox vaccine. This group represents a critical challenge for public health strategies, as they remain unprotected while simultaneously exhibiting lower responsiveness to conventional vaccination messaging. In our sample, individuals with low vaccination likelihood reported significantly lower concern about contracting mpox, as well as lower perceived risk and severity of infection, and were more likely to view mpox as little or not at all problematic in terms of social consequences. In addition, this group demonstrated lower levels of mpox-related knowledge, and more frequently expressed disagreement or neutrality toward recommended prevention strategies. These findings are consistent with previous research showing that individuals who are vaccinated or willing to be vaccinated tend to be better informed about mpox than those who exhibit vaccine hesitancy or unwillingness.32,33
This is the first nationwide study in Spain to assess mpox vaccine uptake and likelihood to vaccinate among GBMSM, expanding beyond prior regional research focused mainly on sociodemographic and clinical aspects.34 In contrast, our study includes a broader national sample and integrates psychosocial, stigma-related, health, and behavioural variables, offering a more comprehensive description of vaccine-related dynamics in this population. This distinction is crucial for understanding the motivational versus structural factors associated with vaccination and the intention–behaviour gap in health behaviour theory.
Despite these strengths, several limitations should be acknowledged. First, the overall sample size, while adequate for primary analyses, limits the statistical power for subgroup analyses, particularly those related to the second objective of the study, which focused on individuals expressing lower likelihood to vaccinate. The small size of this reference group constrains the generalizability of findings and may limit the identification of significant associations. Another potential limitation is the non-probabilistic nature of the sample, which may lead to selection bias. Individuals with greater digital access, higher digital and health literacy, higher engagement with health services, higher educational and economical level, or stronger connections to community networks could be overrepresented, and therefore more likely to be vaccinated, potentially leading to an overestimation of mpox vaccination uptake in our sample. For these reasons, self-reported vaccination coverage in this study should not be interpreted as a population-level estimate. Instead, it must be contextualized within the specific target population for vaccination —namely, individuals eligible for the vaccine due to their high-risk sexual practices and lack of prior immunity (either from smallpox vaccination or previous mpox infection). Additionally, the use of a convenience sample with a limited sample size means that the study population is not representative of the broader Spanish GBMSM population. These limitations should be considered when interpreting the results.
Moreover, the cross-sectional design of the study precludes any inference of causality. Furthermore, as with many self-reported surveys, the possibility of information bias (such as social desirability or recall bias) must be considered, especially given the sensitive nature of the topic. Lastly, the data were collected during a specific moment of the outbreak, and vaccination dynamics may evolve over time depending on epidemiological trends, policy shifts, or changes in public perception, limiting the temporal generalizability of the findings.
Nonetheless, the insights derived from this study are timely and actionable, and they highlight areas that may inform tailored public health strategies that address both vaccination willingness and barriers related to translating intention into action. This suggests the relevance of considering both motivational components (through comprehensive and non-stigmatizing communication led by trusted healthcare professionals) and structural barriers, including stigma, socioeconomic disadvantage, and territorial disparities in healthcare access. Addressing these challenges is essential to ensure equitable vaccine access and to reduce the persistent gap between intention and behaviour in the context of mpox prevention.
Vaccination campaigns targeting GBMSM may play a role in addressing the intention-behaviour gap. Based on our findings and existing literature, several key recommendations can be made to enhance these efforts. Firstly, communication strategies should be led by trusted sources by the GBMSM community, particularly healthcare professionals, official public health institutions, community-based organisations and NGOs, as receiving information from these actors was positively associated with vaccine uptake in our study and others.10,22,29 Messaging from credible and reliable sources has been described as enhancing trust and counteract misinformation, especially in communities that may face systemic marginalization.
Secondly, addressing structural barriers requires a multidimensional approach, such as Tanahashi's framework,14 which defines access through geographic accessibility, acceptability, and appropriateness. In rural or less urbanized areas, lower uptake may reflect not only scarce specialized services (geographic accessibility) but also significant challenges in acceptability. In these settings, the fear of stigma is compounded by institutional stigma and unintentional discrimination within healthcare systems, where a lack of anonymity can deter individuals from disclosing high-risk behaviors or requesting vaccination.28,35
As emphasized in the Spanish Strategic Plan for the Prevention and Control of HIV and STI 2021–2030, addressing these systemic biases is essential to improve prevention efforts.36 Consequently, strategies must go beyond proximity; they must ensure confidentiality and staff training to create stigma-free environments. Implementing mobile clinics and community-led outreach in partnership with NGO could provide more discreet “low-threshold” access points, effectively bridging the gap between vaccination intention and actual behavior in marginalized or less urbanized contexts.22 However, the use of non-habitual vaccination settings also entails logistical challenges, including ensuring adequate cold-chain management, standardized clinical protocols, trained personnel, and integration with existing health information systems for dose registration and follow-up. Addressing these operational considerations is essential to maximize the effectiveness and sustainability of community-based vaccination strategies.
Nevertheless, our findings suggest that low vaccination likelihood among unvaccinated individuals may be driven by broader motivational factors and information regarding mpox rather than by structural barriers alone. In this context, expanding vaccine availability is unlikely to be sufficient to substantially increase uptake in this group. Consequently, interventions aimed at increasing vaccine uptake among individuals with low likelihood of vaccination should prioritize improving the availability, clarity, and relevance of mpox-related information.24 Moreover, further research is needed to better understand the information sources they rely on, their engagement with LGBTIQ+community organizations, and other potential informational barriers that may limit exposure to preventive messaging.
Finally, information campaigns must be comprehensive and clearly explain the risks of infection and the benefits of vaccination, while avoiding stigmatizing language or moralizing tones.24 It is critical that these campaigns do not reinforce negative stereotypes about GBMSM but instead promote a rights-based, inclusive approach that encourages preventive health behaviours without fear or shame.22
ConclusionsIn this first national-level analysis of mpox vaccination among GBMSM in Spain, uptake was reported at 38.0%, while 91.7% of those unvaccinated indicated a high intention to receive the vaccine. There is a substantial gap between actual vaccination and expressed intention among the unvaccinated. While structural and behavioural factors (such as age, urbanicity, PrEP use, and sexual activity) were associated with vaccine uptake, likelihood to vaccinate was primarily associated with psychosocial perceptions, including concern about mpox and perceived severity of infection. These findings highlight the relevance of considering both motivational and structural barriers to vaccination. Enhancing communication through trusted health professionals, expanding access in less urbanised areas, and combating stigma may represent relevant strategies to address barriers related to translating intention into action. Furthermore, interventions should adopt a rights-based, community-informed approach that promotes equity and avoids reinforcing stereotypes. Such efforts are essential to ensure that high-risk populations are not left behind in future public health responses.
Availability of databases and material for replicationThe datasets generated during the current study are not publicly available due to the legal and data protection restrictions established in the inter-institutional collaboration agreement of the LIBERO-POX project. However, they are available from the corresponding author upon reasonable request, subject to the presentation of a formal analysis proposal and approval by the project's Steering Committee.
During the 2022 mpox outbreak, vaccination was key to controlling the infection. However, there is little evidence regarding vaccination uptake and intention to be vaccinated among gay, bisexual and other men who have sex with men in the Spanish context.
What does this study add to the literature?The study provides data on the sociodemographic, psychosocial and behavioural factors associated with vaccination uptake and intention among GBMSM in Spain.
What are the implications of the results?The gap between vaccination intention and uptake requires strategies that address structural barriers and ensure equitable access to vaccination.
Rocío Zurriaga-Carda.
Transparency declarationThe corresponding author, on behalf of the other authors guarantee the accuracy, transparency and honesty of the data and information contained in the study, that no relevant information has been omitted and that all discrepancies between authors have been adequately resolved and described.
Authorship contributionsThe authors confirm that we meet the criteria for authorship. Conceptualization and study design: H. González-Casals and C. Folch. Data collection and analysis: H. González-Casals, H. Martínez-Riveros, N. Lorente, L. Villegas, J. Mena, O. Apffel-Font, J. Casabona, P. Meireles and C. Folch. Writing, original draft: H. González-Casals. Writing, review and editing: H. González-Casals, H. Martínez-Riveros, N. Lorente, L. Villegas, J. Mena, O. Apffel-Font, J. Casabona, P. Meireles and C. Folch. Final approval of the version to be submitted: H. González-Casals, H. Martínez-Riveros, N. Lorente, L. Villegas, J. Mena, O. Apffel-Font, J. Casabona, P. Meireles y C. Folch. Each author has contributed substantially to the work, has reviewed and approved the final version of the manuscript, and agrees to be accountable for all aspects of the work to ensure that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
FundingNone.
Conflicts of interestNone.
LIBERO-POX has been possible thanks to contributions in the form of human, intellectual and economic resources of the member institutions of the RIGHT PLUS Network (Red Iberoamericana de Estudios en Hombres Gay, otros Hombres que tienen Sexo con Hombres y Personas Trans), where the Instituto de Saúde Pública da Universidade do Porto assumed the economic and legal aspects of hosting the database. Thank you to Kai J. Jonas and his group from Maastricht University's Faculty of Psychology and Neuroscience, who provided the questionnaire implemented in a cohort from the Netherlands to serve as the basis for LIBERO-POX's questionnaire. LIBERO-POX was also possible thanks to the support of the collaborating partners in each of the participating countries. Thanks to Grindr© who sent instant promotional messages to their users for free in some of the countries and the Universidad Cayetano Heredia for their economic support in some others.














