





This study investigates the application of the synthetic control method for the evaluation of public health policies, specifically assessing the impact of the 2010 anti-smoking legislation in Spain. This policy, which represented a paradigmatic shift, aimed to reduce smoking prevalence and its multiple consequences for public health. Utilizing data on tobacco consumption prevalence across various countries alongside key predictors of consumption, we examine the effectiveness of the legislation in reducing smoking rates. To achieve this, the synthetic control method is employed to construct a ‘synthetic Spain’ from a weighted combination of countries within a donor pool. This counterfactual represents the smoking prevalence that would have been observed in Spain in the absence of the law. The empirical results demonstrate that the legislation successfully reduced tobacco consumption. However, its gender-differentiated impact suggests the necessity of implementing gender-responsive regulatory frameworks.
Este estudio investiga la aplicación del método de control sintético para la evaluación de políticas de salud pública, específicamente, se evalúa el impacto de la legislación antitabaco de 2010 en España. Esta política, que representó un cambio paradigmático, tenía como objetivo reducir el tabaquismo y sus múltiples consecuencias para la salud pública. Utilizando datos sobre prevalencia del consumo de tabaco en diversos países, junto con predictores clave de consumo, se examina la eficacia de la legislación en la reducción del tabaquismo. Para ello, mediante el método de control sintético, se construye una “España sintética” a partir de la combinación ponderada de los países de un grupo de donantes (donor pool). Este contrafactual representa la prevalencia de consumo que se habría observado en España en ausencia de la ley. Los resultados demuestran que la legislación redujo el consumo de tabaco. Sin embargo, su impacto diferenciado por género sugiere la necesidad de implementar marcos normativos con perspectiva de género.
Tobacco use is the leading cause of preventable death worldwide, generating substantial health losses and social costs through its contribution to cancer, cardiovascular and respiratory diseases.1–3 Beyond its direct health impact, tobacco also imposes environmental and economic burdens, reinforcing the case for strong public regulation.4,5 In Europe, around one quarter of adults smoke, with marked regional differences, which underscores the need for robust and context-sensitive tobacco control policies.6
Public intervention in tobacco consumption is justified by both market failures and individual concerns. Negative externalities —through second-hand smoke and higher public health expenditure— coexist with negative internalities linked to addiction, imperfect information and time-inconsistent preferences.7–10 In response, the WHO Framework Convention on Tobacco Control (FCTC) and the MPOWER package have provided a global blueprint for comprehensive tobacco control, combining price measures, smoke-free regulations, support for cessation, information campaigns, and restrictions on marketing.3,11 Within this framework, the European Union has implemented directives on tobacco products and excise duties, promoting stricter regulation of manufacture, presentation and taxation of tobacco and related products.12,13
Spain has been an active adopter of these recommendations. Law 28/2005 introduced health measures against smoking, regulating the sale, supply, consumption and advertising of tobacco products, and established smoke-free environments in workplaces and certain public spaces. This framework was substantially strengthened by Law 42/2010, which extended the smoking ban to all enclosed public spaces, including bars and restaurants, and tightened restrictions on advertising and sales, aligning Spanish regulation more closely with FCTC and EU guidance.14,15 Evidence suggests that Law 42/2010 has had a stronger impact than the earlier partial ban, contributing to reductions in smoking prevalence, cigarette sales and tobacco-related health outcomes.16–19 At the same time, recent analyses argue that Spanish tobacco control may be lagging behind emerging challenges, and public support for further measures is heterogeneous across regions and types of regulation.20,21
In particular, recent survey evidence for the adult Spanish population shows high acceptability of banning smoking in cars with minors or pregnant women, but substantially lower and more heterogeneous support for more intrusive measures affecting accessibility, such as limiting points of sale, increasing the minimum legal age for tobacco sales to 21 years, or extending smoke-free rules to additional outdoor spaces.22 This pattern suggests that the feasibility of more restrictive policies in Spain depends not only on legal and institutional design, but also specific social norms and attitudes towards tobacco control. Evaluating the actual impact of existing regulations, and understanding which groups benefit most, is thus a prerequisite for designing the next generation of measures.
In this sense, tobacco control policies that are formally gender-neutral can yield uneven outcomes. Gender-blind interventions may reduce overall prevalence while failing to address gender-specific determinants of smoking, such as targeted marketing portraying female smoking as a symbol of emancipation and attractiveness, or gendered stress-coping norms and caregiving roles that shape cessation behaviour.23–25 Prior research indicates that women often benefit more from autonomy-supportive, tailored interventions, whereas men respond more strongly to restrictive regulations, suggesting that neutral designs can inadvertently reinforce existing disparities.3
This study contributes to this literature by evaluating the impact of Spain's 2010 anti-tobacco legislation (Law 42/2010) on smoking prevalence using the synthetic control method, with an explicit gender perspective. By constructing counterfactual trajectories for overall, male and female smoking prevalence, the analysis assesses whether a comprehensive but gender-neutral policy has heterogeneous effects across gender groups. In doing so, it responds to calls for gender-responsive frameworks in tobacco control and aims to inform the design of future regulations that combine effectiveness with equity, in a context where both institutional commitments and public acceptability set important constraints for policy innovation.
MethodThe empirical strategy relies on the synthetic control method (SCM) to estimate the causal impact of Spain's 2010 anti-tobacco legislation (Law 42/2010) on smoking prevalence. Spain is the “treated unit”, and a synthetic counterfactual is constructed as a weighted combination of countries that did not implement comparable legislation at the same time. The weights are chosen so that synthetic Spain reproduces as closely as possible the pre-intervention trajectory of smoking prevalence and key predictors over 1990–2010, and the post-2010 gap between real and synthetic Spain is interpreted as the effect of the law on smoking prevalence. Separate models are estimated for the total population, men and women. The SCM is implemented using standard routines in R, following Abadie and Gardeazábal26 and subsequent extensions,27,28 to which the reader is referred for technical details.
The outcome variable is smoking prevalence, which reflects the age-standardised proportion of individuals using any smoked tobacco daily or occasionally from Global Burden of Disease estimates.29 Data is available for 204 countries (1990–2019), providing consistent annual data by gender. This is preferable for SCM despite being modelled, as national health surveys lack the balanced, harmonised panel structure required. IHME estimates synthesize multiple data sources, which inherently embed differences in survey instruments and sampling frames.29,30 However, in the context of cross-national comparative research, this synthesis is precisely the primary strength of the GBD dataset, because it provides systematically modelled estimates for a large set of countries and years using a unified framework. The donor pool comprises high/middle-income countries without contemporaneous tobacco reforms, based on existing comparative evidence on European and international tobacco regulation.31,32
The predictor set includes a parsimonious group of determinants of smoking prevalence. First, following Abadie et al.27 we incorporate alcohol use disorders, which accounts for the current number of cases per 100 people.33 Second, excise tax serves as a strong proxy for countries’ overall fiscal–regulatory stance towards harmful consumption.14,34 Third, health spending (per capita) and smoking–attributable mortality per 100,000 people (death rate) to capture health system resources and the burden of tobacco–related morbidity and mortality. Fourth, socioeconomic conditions are represented by OECD's tertiary education (25–34 years) indicator, Unemployment rate, and the adjusted net national income (per capita), which reflect the well–documented links between educational attainment, labour market status, income and smoking behaviour.35–38. Finally, Suicide ratio is included as a proxy for mental health and psychosocial stressors, which are often associated with higher tobacco use. Following Abadie39 and Ben-Michael et al.40, lagged outcome values (smoking prevalence in 1996, 2001 and 2009) are included to improve pre-intervention fit and ensure that unobserved confounders correlated with past trends are captured by the synthetic control.
In the SCM, predictors are typically assumed to be exogenous, capturing stable pre-treatment characteristics unaffected by the intervention. For any potentially endogenous predictors, their inclusion is justified in the literature as they enhance approximation of unobserved heterogeneity when pre-treatment data is sufficiently rich, as formalized in Abadie et al.27 and extended under sequential exogeneity assumptions. Thus, our predictors satisfy these conditions, ensuring valid counterfactual construction.
Model adequacy is assessed through the pre-intervention goodness of fit and a battery of standard robustness checks. These include leave-one-out exercises, in which donor countries with positive weights are iteratively excluded to test the sensitivity of the estimated effect, and placebo tests that reassign the intervention to each control country in turn, comparing Spain's post/pre mean squared prediction error (MSPE) ratio to the distribution of placebo MSPE ratios. A statistically meaningful impact of Law 42/2010 is inferred when Spain exhibits both a close pre-intervention fit and a distinctly larger post-intervention divergence from its synthetic counterpart than those observed in placebo units.
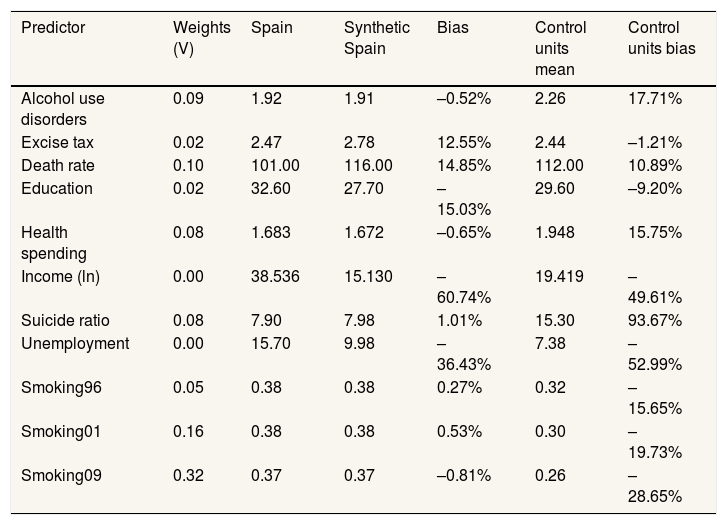
ResultsTable 1 summarises the predictors used in the synthetic control construction and their balance between Spain and synthetic Spain in 2011. Key predictors of smoking behaviour (lagged prevalence in 1996, 2001 and 2009) display negligible bias, similar to the findings of Abadie et al.27. Reliance on these predictors strengthens the validity of the model by replicating smoking trends in the treated country. Remaining covariates show moderate differences that are substantially smaller than those observed between Spain and the unweighted average of donor countries. This pattern indicates that the synthetic control reproduces Spain's pre-intervention characteristics more closely than the simple donor mean and supports the adequacy of the predictor set.40
Weights and values of the predictors used for synthetic control in 2011.
| Predictor | Weights (V) | Spain | Synthetic Spain | Bias | Control units mean | Control units bias |
|---|---|---|---|---|---|---|
| Alcohol use disorders | 0.09 | 1.92 | 1.91 | –0.52% | 2.26 | 17.71% |
| Excise tax | 0.02 | 2.47 | 2.78 | 12.55% | 2.44 | –1.21% |
| Death rate | 0.10 | 101.00 | 116.00 | 14.85% | 112.00 | 10.89% |
| Education | 0.02 | 32.60 | 27.70 | –15.03% | 29.60 | –9.20% |
| Health spending | 0.08 | 1.683 | 1.672 | –0.65% | 1.948 | 15.75% |
| Income (ln) | 0.00 | 38.536 | 15.130 | –60.74% | 19.419 | –49.61% |
| Suicide ratio | 0.08 | 7.90 | 7.98 | 1.01% | 15.30 | 93.67% |
| Unemployment | 0.00 | 15.70 | 9.98 | –36.43% | 7.38 | –52.99% |
| Smoking96 | 0.05 | 0.38 | 0.38 | 0.27% | 0.32 | –15.65% |
| Smoking01 | 0.16 | 0.38 | 0.38 | 0.53% | 0.30 | –19.73% |
| Smoking09 | 0.32 | 0.37 | 0.37 | –0.81% | 0.26 | –28.65% |
The large difference between the average of the control units in some predictors and their value in real Spain (suicide rate or unemployment) suggests that the country is a relatively unique case in some aspects. This reinforces the usefulness of the synthetic control to generate a more accurate counterfactual by not relying solely on the average of the control units but on a weighted combination of several countries. The synthetic control method thereby safeguards against estimating extreme counterfactuals, that is, those that protrude from the convex hull of the data.41 Thus, all definite and diagonal matrices are chosen to minimise the mean squared prediction error of the prevalence of tobacco consumption in Spain during the period prior to the intervention.
Spain's tobacco consumption trends are optimally reproduced by Greece (0.63), Israel (0.14), Chile (0.07), Switzerland (0.06), Finland (0.05), Lithuania (0.03), Slovenia (0.02), and Colombia (0.004), while the rest of the countries are assigned a value of zero.
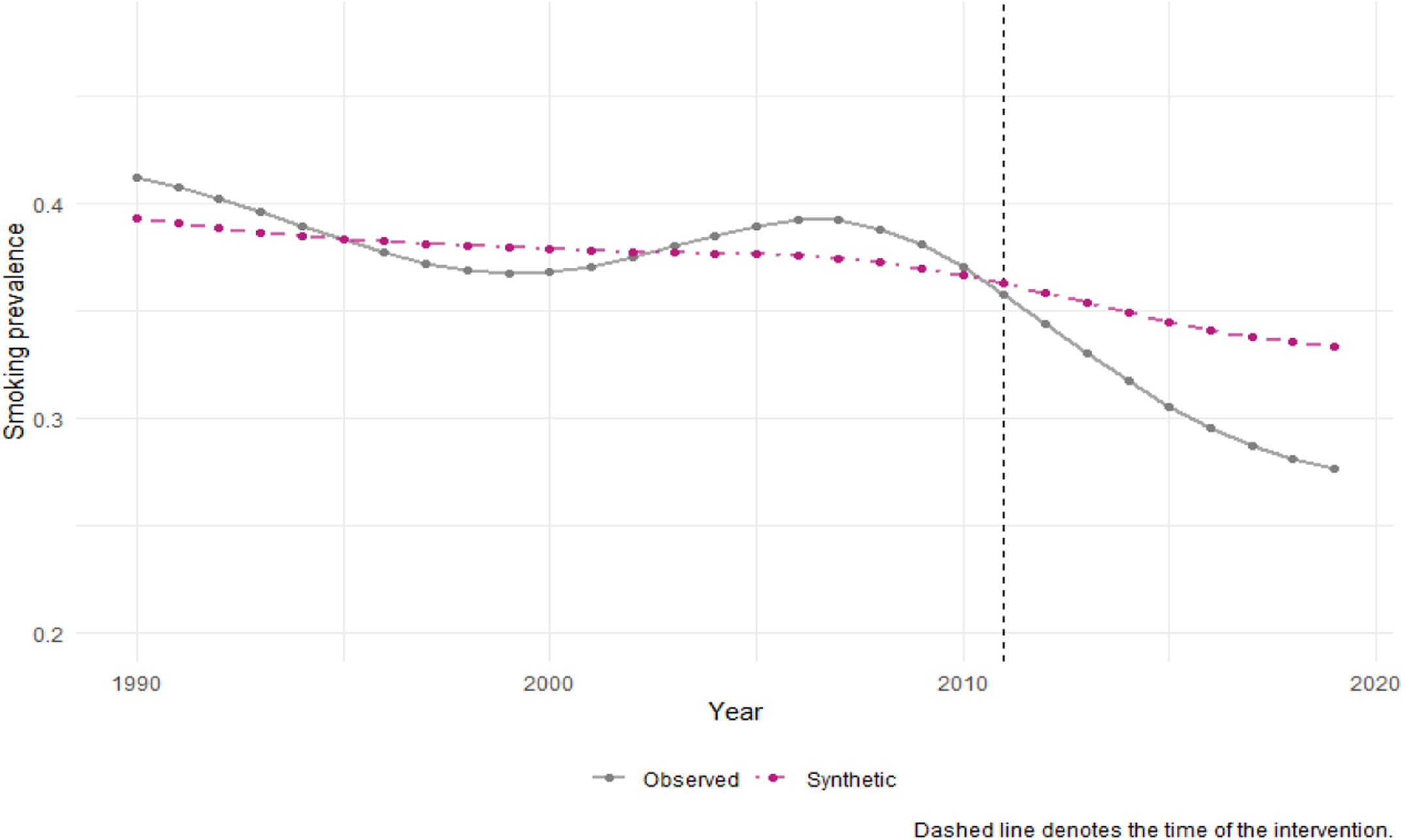
Figure 1 shows the trajectory of age-standardised smoking prevalence for Spain and its synthetic counterpart for the total population between 1990 and 2019. The pre-intervention fit is very close, suggesting that the SCM provides a credible approximation to the counterfactual path in the absence of Law 42/2010. After the law came into force, observed prevalence in Spain declines more rapidly than in synthetic Spain, and the gap widens progressively over time.

Figure 2 makes this effect more explicit by plotting the difference between Spain and synthetic Spain: from 2010 onwards, the estimated effect becomes negative and reaches a sizeable reduction in smoking prevalence by the end of the period, consistent with a delayed but sustained impact of comprehensive smoke-free legislation.42 We have replicated the analysis by re-estimating the SCM excluding potentially endogenous predictors (such as alcohol use disorders and suicide rates). The results demonstrate that the estimated impact of Law 42/2010 remains remarkably stable and does not change substantially with this restricted set of variables, confirming that our primary findings are not an artifact of endogeneity in the weight-selection step (see Supplementary material online).

The increase in the line in 2005 can be interpreted as the initial stubbornness of smokers (rebound effect), which undergoes course correction in the longer term, culminating in modification of behaviour, reflected by the eventual decline in the prevalence. This idea is supported by Cotti et al.43 and Smith and Malone,44 which examine the rebound effect of tobacco control policies.
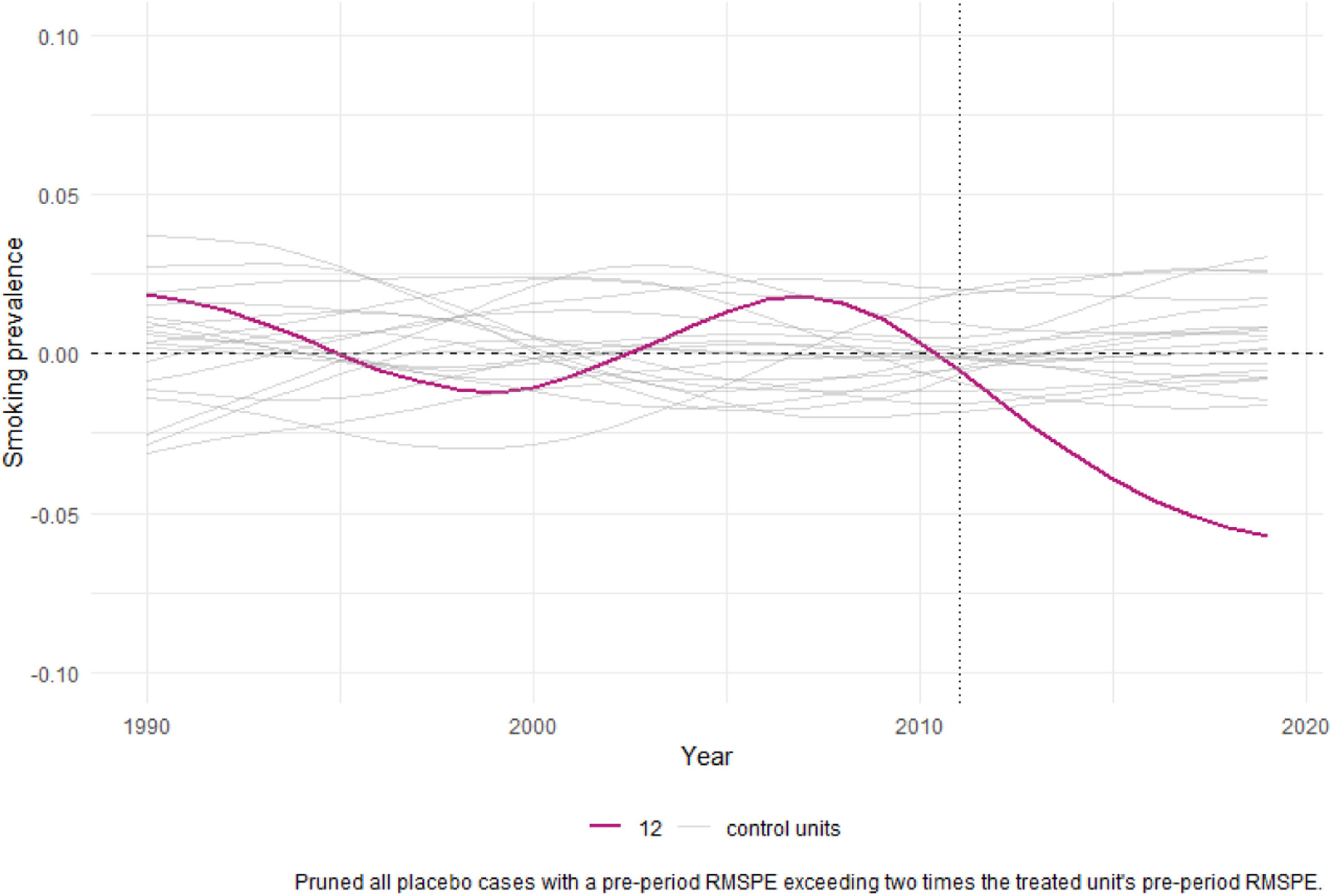
The robustness of these findings is examined in figure 3, which presents a placebo test for the total population model. When the intervention date is reassigned to each donor country and synthetic controls are re-estimated, the gaps observed for placebo units fluctuate around zero and do not exhibit a systematic post-2010 divergence. In contrast, Spain's line shows a pronounced and persistent reduction in smoking prevalence relative to its synthetic control after 2010. The post-/pre-intervention MSPE ratio places Spain in the lower tail of the placebo distribution, with a p-value of approximately 0.08, indicating that an effect of this magnitude is unlikely to be driven by random variation alone.28

Leave-one-out (LOO) exercises confirm that the estimated impact is not driven by any single donor country with extreme smoking patterns. Greece emerges as the country with the greatest weight in synthetic Spain, with its minimum tobacco prevalence values higher than the maximum values of the rest of the countries. When it is excluded from the base to carry out the LOO test, it does not alter the evidence as it shows similar results in the iterations.
The p-value was calculated by comparing the post/pre-treatment MSPE ratio for the treated unit against the distribution of MSPE ratios from placebo units (untreated units). A p-value of 0.083 obtained from the placebo test (MSPE ratio test) indicates that the probability of observing an effect as extreme as that of the treated unit by chance is 8.3%.
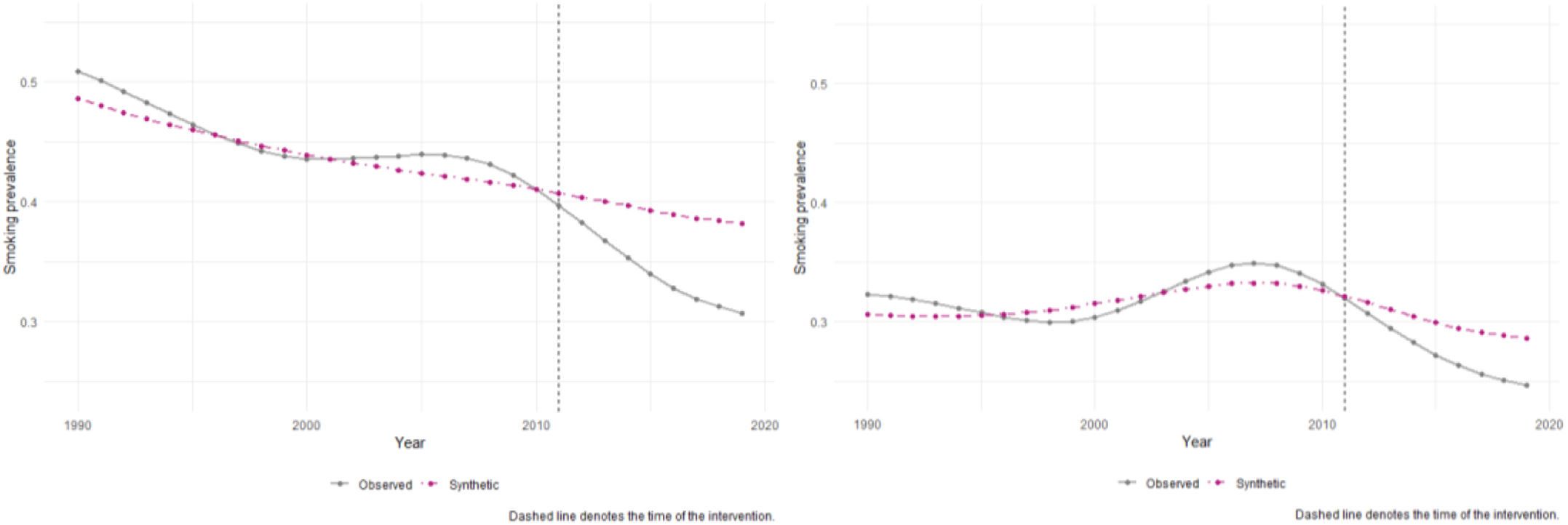
The gender-disaggregated analysis reveals marked gender heterogeneity. Figure 4 display smoking prevalence for men and women in Spain and their respective synthetic controls; in both cases, the pre-2010 fit is satisfactory. For men, the observed series diverges sharply from synthetic Spain after the law's implementation, with a reduction exceeding 20 percentage points over the full observation window. For women, the divergence is much smaller. It shows a large and persistent negative effect for men, while the estimated reduction for women, as seen in figure 4, remains modest (around two percentage points) and does not clearly separate from zero. Placebo-based inference indicates a statistically significant effect for men (post-/pre-MSPE p ≈ 0.04) but not for women, suggesting that Law 42/2010 had a substantial impact on male smoking prevalence, whereas its effect on female smoking behaviour was weaker and statistically less robust.45,46
Discussion and conclusions
Smoking has been a global concern for decades. In line with the health-related sustainable development goals of the World Health Organization (WHO), a wide range of measures have been implemented by countries over the years to promote smoke-free spaces and discourage tobacco consumption among the population. Recently, tobacco prevention organisations from 15 European countries have begun collecting signatures in support of the European Citizens’ Initiative, which aims to progressively abolish the sale of tobacco and nicotine and achieve a generation free of smoke by 2030.47
In Spain, there have been two key policies in this regard: Law 28/2005 on health measures against smoking and regulating the sale, supply, consumption and advertising of tobacco products, and Law 42/2010, which extended the smoking ban to bars and restaurants, and tightened advertising and sales restrictions. Evidence has shown that the latter was the more effective of the two.16–18,48
Our results show that Spain's 2010 anti-tobacco legislation significantly reduced smoking prevalence overall, but with starkly divergent gender outcomes. However, the observed decline in smoking prevalence should be interpreted as the impact of a broader regulatory framework since other laws besides Law 42/2010 began to be implemented shortly thereafter, such as Law 1/2011, although, for instance, the latter applied specifically to the Canary Islands. The synthetic control analysis reveals a significant reduction among men, contrasting with a marginal, statistically non-significant reduction of 2.1 percentage points among women. This gender gap mirrors broader European trends, where tobacco control policies often yield weaker effects for women, particularly in Mediterranean contexts.45,49
The legislation's limited impact on women stems from intersecting social, economic, and biological factors. Targeted tobacco industry marketing has historically linked female smoking to emancipation and beauty ideals, undermining gender-neutral policies.45 Undoubtedly, the tobacco industry has successfully incorporated this perspective in its promotional campaigns aimed at women, such as with Virginia Slim cigarettes, which capitalised on “changes in social attitudes towards women by promoting smoking as a symbol of emancipation”.50,51 The impact of social media and products such as e-cigarettes in recent times must be taken into account too.52,53
Concurrently, socioeconomic vulnerability —especially among low-educated women, who exhibit 30% higher smoking persistence post-2010— exacerbates cessation barriers due to caregiving burdens and limited access to tailored support.46 Although women smoke less than men, they tend to smoke milder varieties, which conditions their risk perception and decisions, consequently resulting in a lower cessation rate among them.54–56
Public policies must incorporate a gendered perspective both in the analysis of the problem and in the approach to tobacco control interventions in order to achieve progress in reducing the prevalence of consumption. Some interventions of this nature have already been in place in countries like Bangladesh and India. Awareness campaigns here focus on the risks of smokeless tobacco and are carried out specifically targeting women, using communication channels and messages adapted to their cultural context. Support programmes to quit smoking are channelled through female leaders and women's groups in the dissemination of messages.57
To address these disparities, future policies must adopt comprehensive gender-responsive strategies. This includes implementing tailored interventions such as autonomy-supportive programs that specifically address women's motivations, for example, by focusing on disease prevention and emphasizing the importance of role-modelling healthy behaviours for children. Additionally, providing group-based psychological support can help women navigate gender-specific stressors. Structural reforms are also essential; integrating childcare subsidies would reduce barriers to participation, while banning gender-targeted marketing and funding counter-messaging initiatives in the media could help dismantle harmful stereotypes. Finally, enhanced monitoring through the systematic collection of sex-disaggregated data is necessary to ensure that policy outcomes are equitable and to inform ongoing improvements.
In conclusion, Spain's experience underscores that gender-blind tobacco control perpetuates inequities and undermines United Nations’ sustainable development goals 3 and 5, related to health and gender equality. Even though this has been highlighted in policy debates for some years now, initiatives have been few and far between.58,59 Achieving the WHO's “tobacco-free generation” goal by 2030 requires embedding gender-specific mechanisms —from industry tactics to biological vulnerabilities— into policy design. Only through such nuanced approaches can public health initiatives ensure equitable reductions in smoking prevalence across all demographics.
Comprehensive smoke free laws reduce smoking and tobacco related harm, but evidence on their long term, gender differentiated effects in Europe remains limited and is based on few longitudinal or quasi experimental evaluations (WHO, 2021).
What does this study add to the literature?It applies the synthetic control method to Spain's 2010 smoke free law and shows that the reduction in smoking prevalence is substantially larger for men than for women.
What are the implications of the results?Findings indicate that formally gender neutral tobacco control can widen gender gaps, underscoring the need for explicitly gender responsive policies, monitoring and cessation support.
All data used in this study are publicly available and accessible. The sources of the data are cited throughout the article.
Editor in chargeMiquel Serra-Burriel.
Transparency declarationThe corresponding author, on behalf of the other authors guarantee the accuracy, transparency and honesty of the data and information contained in the study, that no relevant information has been omitted and that all discrepancies between authors have been adequately resolved and described.
Authorship contributionsAll authors contributed to the conception and design of the study, analysis and interpretation of data, drafting and critical revision of the manuscript. All authors approved the final version of the manuscript.
FundingThis research was funded by the Conselleria d’Hisenda i Model Econòmic in Generalitat Valenciana project HIECPU/2022/5.
Conflicts of interestNone.












