



To describe food consumption frequency in adolescents in the context of the financial crisis in 2012, and to analyse potential fluctuations in excess body weight between 2008 and 2012.
MethodA cross-sectional study of eating habits and excess body weight was conducted in adolescents aged 13 to 19 years old from public, subsidised and private secondary schools in Barcelona, Spain. The FRESC lifestyle risk factors survey was used, and food frequency consumption, food recommendations and body mass index were analysed according to gender, year of education and socioeconomic status.
ResultsGirls ate vegetables and fruits more frequently than boys, while the prevalence of junk food consumption was higher in boys. The prevalence of compliance with food recommendations was lower than 50% for all foods, and gender and socioeconomic differences were found for eggs, red meat and soft drinks. Regarding excess body weight, boys had a higher prevalence than girls in the 2 years analysed. Furthermore, a reduction in excess body weight was observed among girls in secondary education in the highest socioeconomic groups (28.7% [95% CI: 24.8-32.6%] in 2008 to 20.5% [95% CI: 17.1-23.8%] in 2012).
ConclusionsThe prevalence of adolescents following food recommendations is low, and gender differences were found in terms of food consumption frequency, even in the context of financial crisis. There is a need to promote programmes and policies to reduce inequalities related to eating habits and excess body weight in adolescents.
Describir la frecuencia de consumo de alimentos en adolescentes en un contexto de crisis económica en el año 2012, y analizar los potenciales cambios en el exceso de peso entre los años 2008 y 2012.
DiseñoEstudio transversal de los hábitos alimentarios y el exceso de peso en adolescentes de entre 13 y 19 años de edad pertenecientes a escuelas públicas, concertadas y privadas de Barcelona. Se utilizó la encuesta FRESC sobre factores de riesgo asociados a estilos de vida y se analizaron, según sexo, curso académico y nivel socioeconómico, las frecuencias de consumo, recomendaciones alimentarias e índice de masa corporal.
ResultadosLas chicas realizaban un mayor consumo de frutas y verduras, mientras que los chicos consumían comida no saludable con mayor frecuencia. La prevalencia de cumplimiento de las recomendaciones alimentarias es inferior al 50% para todos los alimentos, y se encontraron diferencias según el sexo y el nivel socioeconómico en el consumo de huevos, carne roja y refrescos. En relación al exceso de peso, la prevalencia fue mayor en los chicos que en las chicas en los 2 años analizados. Además, se observó una reducción del exceso de peso en las chicas cursando Educación Secundaria Obligatoria y de nivel socioeconómico alto (de 28,7% [IC95%: 24,8-32,6%] en 2008 a 20,5% [IC95%: 17,1-23,8%] en 2012).
ConclusionesLa prevalencia de adolescentes que siguen las recomendaciones de consumo es baja. Hay diferencias de sexo en las frecuencias de consumo de los alimentos, incluso en un contexto de crisis económica. Existe una necesidad de promover programas y políticas para reducir las desigualdades relacionadas con los hábitos alimentarios y el exceso de peso en los adolescentes.
Excess weight (overweight and obesity) in adolescents is a major concern in Spain due to the high prevalences of overweight and obesity at 17% and 8.5% respectively in 2012.1 Moreover, adolescents with excess weight are more likely to be overweight or obese in adulthood2 and to have a higher risk of cardiovascular diseases3 which are one of the main causes of death in Spain.4 Excess weight is influenced by multiple factors, with eating habits playing a key role.
The “food recommendation pyramid” graphically represents the recommended frequency of food consumption according to their properties.5 In general, a healthy diet should include daily consumption of cereals or potatoes, vegetables, fruits and dairy products; meat, fish and eggs a few times per week; and sausages, sweets and manufactured products only occasionally.5 Eating habits are especially important during adolescence due to the physical and mental development that takes place at this period of life.6 Moreover, in adolescence, some lifestyles can be established and last until later stages, and therefore the acquisition of healthy habits, including eating habits, is especially important.7
The Spanish population has been experiencing an economic crisis since the third trimester of 2008. It is known that economic recessions can modify eating habits and,8,9 despite the lack of scientific published data, the available information from some organizations and non-governmental organizations show that there might be increasing food insecurity.10–12 The Sociologic Investigation Center of Spain and UNICEF reported that eating habits in families might be changing, especially by reducing fresh food consumption, due to families’ limited economic resources.10,12 The Sindic de Greuges, a public organization that defends the fundamental rights of the Catalan population, warned that 2,800 children in Catalonia could have food security problems, and around 50,000 might have insufficient protein intake.11
Published studies on food consumption frequency in adolescents in Spain are limited,13,14 or focus on other eating behaviours.15,16 Since 1987 a lifestyle risk-factor survey (FRESC) has been administered periodically to the adolescent population in Barcelona. The main objectives of this study were to describe eating habits in terms of food consumption frequency and compliance with food recommendations among adolescents in 2012 (in an economic crisis setting), and to analyse changes in the prevalence of excess weight as a health indicator between 2008 (before the economic crisis) and 2012.
MethodsA cross-sectional study based on two representative samples of students from Barcelona was carried out using the 2008 and 2012 FRESC surveys (lifestyle risk-factor survey for secondary school students [FRESC]). Both surveys were administered to adolescents enrolled in the 8th year of education (13-14 years old), 10th year (15-16 years old) and 12th year (17-18 years old) in secondary schools in the city of Barcelona, Spain.17,18
Samples were obtained following the same procedure in each edition of the survey. The sample size was calculated to obtain a 3% precision and assuming 95% confidence for a proportion of 0.5. The sample assessed for each year of education and edition was 1,250 adolescents, taking into account a 20% loss. Classrooms were used as the sample unit and were randomly selected for each year, stratifying by the family economic capacity index (low, medium and high −FECI-96−) and type of school (state, subsidized or private).
The FRESC questionnaire includes sociodemographic information and questions on different health risk factors, such as addictive substances, physical activity, emotional relationships, and food consumption frequency. The questionnaire was anonymous and was administered, with the prior permission of the schools’ headmasters, by professionals from the Public Health Agency of Barcelona (ASPB, Agència de Salut Pública de Barcelona) between the first and second trimester of the year. In 2008 and 2012 editions, students’ weight and height were objectively measured with their prior consent at the end of the questionnaire by the same professionals.
Principals and teachers of selected schools were properly informed about the objectives of the study. Furthermore, they gave their verbal informed consent and arranged a meeting with trained personnel of the ASPB and students for the administration of the questionnaire during regular school hours at classrooms. Students were also informed about the study and that their participation was absolutely voluntary, being free of not answering any question they did not consider appropriate. Students were also guaranteed that their responses were anonymous and would not be treated individually in any case. They were told not to write down their names or other personal identifiers in the questionnaire to assure anonymity. The study was approved by the Research Committee of the ASPB and parental informed consent was not considered necessary given the nature of the questionnaire.
Food consumption frequency was described using the food frequency questionnaire included in the 2012 FRESC survey, which provided data from a context of economic crisis. It was studied in terms of “food consumption frequency” and “compliance with the food recommendations”. Food consumption questions included the following items: bread, rice and pasta, potato or yucca, cereals, raw vegetables, boiled vegetables, fruits, legumes, meat (white and red), sausage, fish, eggs, dairies, nuts, pastries, sweets, milk desserts, crisps, and soft drinks. The response options differed, depending on the food, and ranged from “never or less than once a month” to “at least once a day”. Food consumption frequency was analysed by categorizing the food questions of the survey into “never”, “weekly” and “daily”. “Never” included the answers “never or less than once a month”; “weekly” included between “1 and 3 times a month” and “4 and 6 times a week”; and “daily” included between “once a day” and “3 or more times a day”. Compliance with food recommendations was analysed according to the “food recommendation pyramid”.5 The food answers from the questionnaire which contained the recommended frequency were classified as the “recommended” category for each food. The other categories were classified in “more than recommended” when the frequency was higher than recommended and “less than recommended” when the frequency was lower than recommended when possible. Since the recommendations for bread, rice and pasta, potato or yucca and cereals is for the entire group together, a variable called “carbohydrate” was created by pooling them together. The same was done for the variable “fruit and vegetables”, which included cooked and raw vegetables and fruits. “Junk food” included crisps, milk desserts, sweets and pastries.
Body mass index (BMI) information was extracted from the 2008 (before the economic crisis) and 2012 FRESC surveys. Weight and height were used to calculate the adolescents’ Quetelet index or BMI. The variable created weight status was defined using the age- and sex-specific cut-offs proposed by the World Health Organisation Z-score.19 The categories given were “low weight”, “normal weight”, “overweight” and “obesity” and were recategorized in two categories: “excess weight”, which included “overweight” and “obesity”, and “non-excess weight”, which included low and normal weight.
The sociodemographic variables analysed were age, sex, school year (8th, 10th or 12th year), which was categorized in compulsory education (8th and 10th years) and postcompulsory education (12th year), type of school (state, private or subsidized) and socioeconomic status (SES) based on the family affluence scale (FAS), which is an individual socioeconomic index that reflects family expenditure and consumption by asking for the number of holidays per year, the number of computers and cars at home and the availability of a private bedroom at home.20 The result is a scale that goes from 0 to 9 points, and it can be categorized in three groups: low affluence (0 to 3 points), middle affluence (4 or 5) and high affluence (6 to 9).
Bivariate analyses stratified by sex and year were conducted for “food consumption frequency”. Food consumption recommendations were analysed by FAS and sex (no stratification analysis by year was applied since there were no significant differences between them). In both cases, the chi-squared test with a significance level of 0.05 was used for comparison. Neither food frequency nor food recommendations were possible to compare between 2008 and 2012, since food frequency records differed between both editions. Excess weight data from the 2008 and 2012 FRESC surveys were analysed by comparing the prevalences of the two editions and stratifying them by sex, FAS and year, and using 95% confidence intervals (95%CI) for comparison. All statistical analysis were performed using the software STATA/IC11.2.
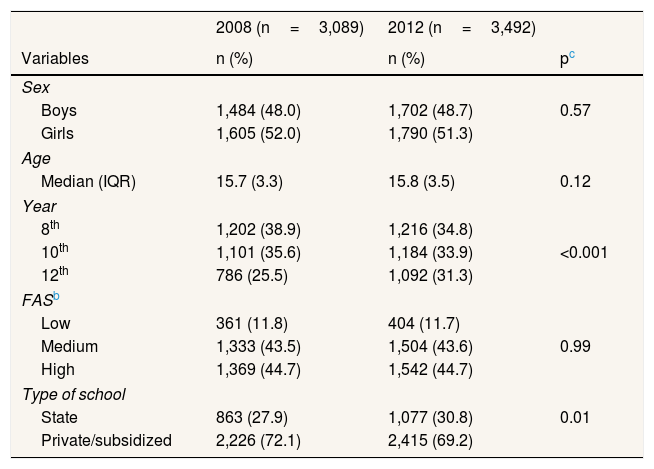
ResultsTable 1 shows the main characteristics of the sample. A total of 3,089 students were analysed in the 2008 survey and 3,492 students in the 2012 survey. Around 48% of the students were boys and the median age was 15.7 years in 2008 and 15.8 years in 2012.
Sociodemographic characteristics of the sample. FRESCa survey 2008 and 2012, Barcelona.
| 2008 (n=3,089) | 2012 (n=3,492) | ||
|---|---|---|---|
| Variables | n (%) | n (%) | pc |
| Sex | |||
| Boys | 1,484 (48.0) | 1,702 (48.7) | 0.57 |
| Girls | 1,605 (52.0) | 1,790 (51.3) | |
| Age | |||
| Median (IQR) | 15.7 (3.3) | 15.8 (3.5) | 0.12 |
| Year | |||
| 8th | 1,202 (38.9) | 1,216 (34.8) | |
| 10th | 1,101 (35.6) | 1,184 (33.9) | <0.001 |
| 12th | 786 (25.5) | 1,092 (31.3) | |
| FASb | |||
| Low | 361 (11.8) | 404 (11.7) | |
| Medium | 1,333 (43.5) | 1,504 (43.6) | 0.99 |
| High | 1,369 (44.7) | 1,542 (44.7) | |
| Type of school | |||
| State | 863 (27.9) | 1,077 (30.8) | 0.01 |
| Private/subsidized | 2,226 (72.1) | 2,415 (69.2) | |
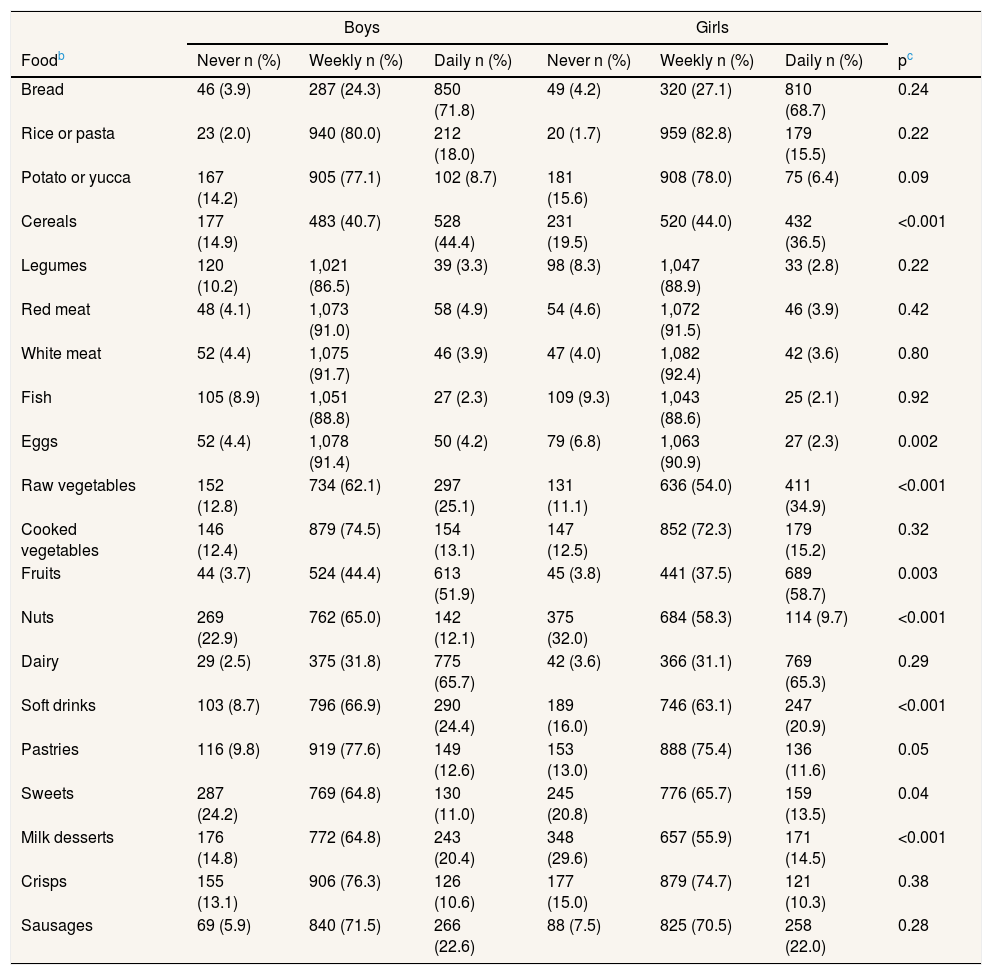
Table 2 shows that boys from the 8th to 10th years ate eggs (4.2%) in a significantly higher daily frequency than girls (2.3%). Boys also showed higher junk food consumption, reporting never eating “milk desserts” (14.8%), “pastries” (9.5%) and “soft drinks” (8.7%) in a lower frequency than girls (29.6%, 13.0% and 16.0% respectively). In contrast, girls showed a significantly higher daily consumption frequency of raw vegetables (34.9%), cooked vegetables (15.2%) and fruits (58.7%) than boys (25.1% ate raw vegetables, 13.1% ate cooked vegetables and 51.9% ate fruits).
Food consumption frequency by sex in the 8th and 10th years. FRESCa survey 2012, Barcelona.
| Boys | Girls | ||||||
|---|---|---|---|---|---|---|---|
| Foodb | Never n (%) | Weekly n (%) | Daily n (%) | Never n (%) | Weekly n (%) | Daily n (%) | pc |
| Bread | 46 (3.9) | 287 (24.3) | 850 (71.8) | 49 (4.2) | 320 (27.1) | 810 (68.7) | 0.24 |
| Rice or pasta | 23 (2.0) | 940 (80.0) | 212 (18.0) | 20 (1.7) | 959 (82.8) | 179 (15.5) | 0.22 |
| Potato or yucca | 167 (14.2) | 905 (77.1) | 102 (8.7) | 181 (15.6) | 908 (78.0) | 75 (6.4) | 0.09 |
| Cereals | 177 (14.9) | 483 (40.7) | 528 (44.4) | 231 (19.5) | 520 (44.0) | 432 (36.5) | <0.001 |
| Legumes | 120 (10.2) | 1,021 (86.5) | 39 (3.3) | 98 (8.3) | 1,047 (88.9) | 33 (2.8) | 0.22 |
| Red meat | 48 (4.1) | 1,073 (91.0) | 58 (4.9) | 54 (4.6) | 1,072 (91.5) | 46 (3.9) | 0.42 |
| White meat | 52 (4.4) | 1,075 (91.7) | 46 (3.9) | 47 (4.0) | 1,082 (92.4) | 42 (3.6) | 0.80 |
| Fish | 105 (8.9) | 1,051 (88.8) | 27 (2.3) | 109 (9.3) | 1,043 (88.6) | 25 (2.1) | 0.92 |
| Eggs | 52 (4.4) | 1,078 (91.4) | 50 (4.2) | 79 (6.8) | 1,063 (90.9) | 27 (2.3) | 0.002 |
| Raw vegetables | 152 (12.8) | 734 (62.1) | 297 (25.1) | 131 (11.1) | 636 (54.0) | 411 (34.9) | <0.001 |
| Cooked vegetables | 146 (12.4) | 879 (74.5) | 154 (13.1) | 147 (12.5) | 852 (72.3) | 179 (15.2) | 0.32 |
| Fruits | 44 (3.7) | 524 (44.4) | 613 (51.9) | 45 (3.8) | 441 (37.5) | 689 (58.7) | 0.003 |
| Nuts | 269 (22.9) | 762 (65.0) | 142 (12.1) | 375 (32.0) | 684 (58.3) | 114 (9.7) | <0.001 |
| Dairy | 29 (2.5) | 375 (31.8) | 775 (65.7) | 42 (3.6) | 366 (31.1) | 769 (65.3) | 0.29 |
| Soft drinks | 103 (8.7) | 796 (66.9) | 290 (24.4) | 189 (16.0) | 746 (63.1) | 247 (20.9) | <0.001 |
| Pastries | 116 (9.8) | 919 (77.6) | 149 (12.6) | 153 (13.0) | 888 (75.4) | 136 (11.6) | 0.05 |
| Sweets | 287 (24.2) | 769 (64.8) | 130 (11.0) | 245 (20.8) | 776 (65.7) | 159 (13.5) | 0.04 |
| Milk desserts | 176 (14.8) | 772 (64.8) | 243 (20.4) | 348 (29.6) | 657 (55.9) | 171 (14.5) | <0.001 |
| Crisps | 155 (13.1) | 906 (76.3) | 126 (10.6) | 177 (15.0) | 879 (74.7) | 121 (10.3) | 0.38 |
| Sausages | 69 (5.9) | 840 (71.5) | 266 (22.6) | 88 (7.5) | 825 (70.5) | 258 (22.0) | 0.28 |
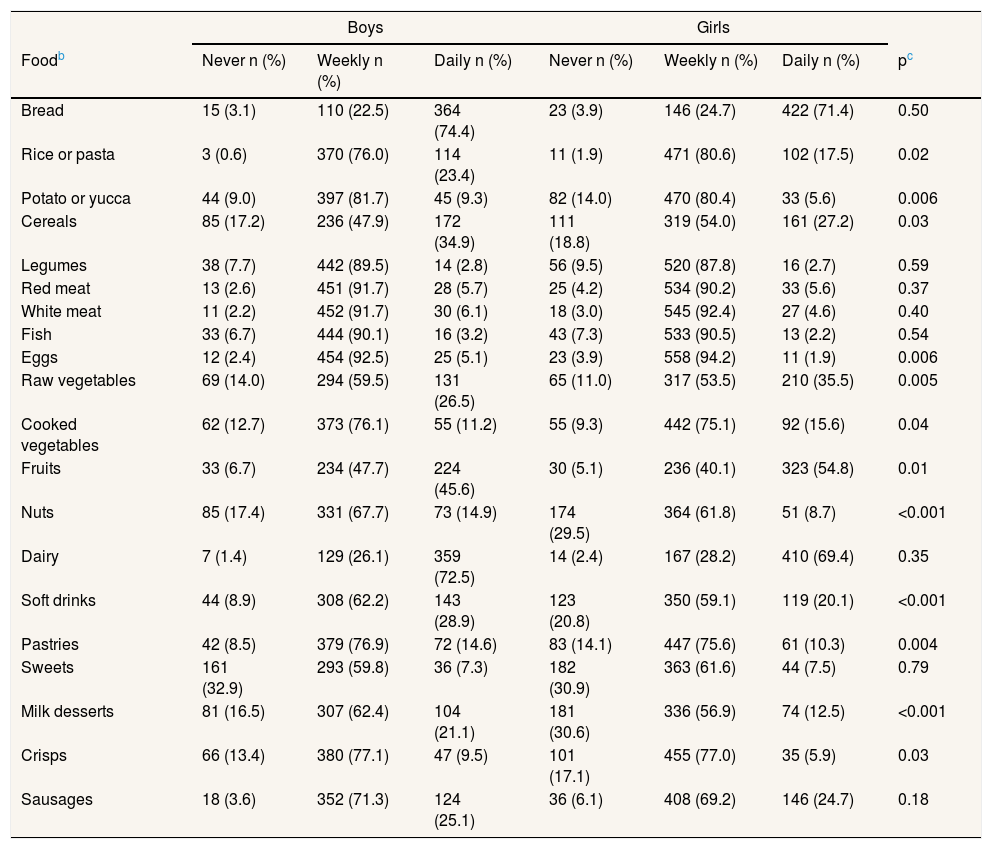
Among adolescents in the 12th year (Table 3), significant differences in daily consumption frequencies were found between boys and girls for raw vegetables (35.5% girls and 26.5% boys), cooked vegetables (15.6% girls 11.2% boys) and fruits (54.8% girls 45.6% boys). As in the group in the 8th to 10th years, boys also showed lower prevalences of “never eating” “milk desserts” (16.5%), “pastries” (8.5%) and “soft drinks” (8.9%) than girls (30.6%, 14.1% and 20.8%, respectively).
Food consumption frequency by sex in the 12th year. FRESCa survey 2012, Barcelona.
| Boys | Girls | ||||||
|---|---|---|---|---|---|---|---|
| Foodb | Never n (%) | Weekly n (%) | Daily n (%) | Never n (%) | Weekly n (%) | Daily n (%) | pc |
| Bread | 15 (3.1) | 110 (22.5) | 364 (74.4) | 23 (3.9) | 146 (24.7) | 422 (71.4) | 0.50 |
| Rice or pasta | 3 (0.6) | 370 (76.0) | 114 (23.4) | 11 (1.9) | 471 (80.6) | 102 (17.5) | 0.02 |
| Potato or yucca | 44 (9.0) | 397 (81.7) | 45 (9.3) | 82 (14.0) | 470 (80.4) | 33 (5.6) | 0.006 |
| Cereals | 85 (17.2) | 236 (47.9) | 172 (34.9) | 111 (18.8) | 319 (54.0) | 161 (27.2) | 0.03 |
| Legumes | 38 (7.7) | 442 (89.5) | 14 (2.8) | 56 (9.5) | 520 (87.8) | 16 (2.7) | 0.59 |
| Red meat | 13 (2.6) | 451 (91.7) | 28 (5.7) | 25 (4.2) | 534 (90.2) | 33 (5.6) | 0.37 |
| White meat | 11 (2.2) | 452 (91.7) | 30 (6.1) | 18 (3.0) | 545 (92.4) | 27 (4.6) | 0.40 |
| Fish | 33 (6.7) | 444 (90.1) | 16 (3.2) | 43 (7.3) | 533 (90.5) | 13 (2.2) | 0.54 |
| Eggs | 12 (2.4) | 454 (92.5) | 25 (5.1) | 23 (3.9) | 558 (94.2) | 11 (1.9) | 0.006 |
| Raw vegetables | 69 (14.0) | 294 (59.5) | 131 (26.5) | 65 (11.0) | 317 (53.5) | 210 (35.5) | 0.005 |
| Cooked vegetables | 62 (12.7) | 373 (76.1) | 55 (11.2) | 55 (9.3) | 442 (75.1) | 92 (15.6) | 0.04 |
| Fruits | 33 (6.7) | 234 (47.7) | 224 (45.6) | 30 (5.1) | 236 (40.1) | 323 (54.8) | 0.01 |
| Nuts | 85 (17.4) | 331 (67.7) | 73 (14.9) | 174 (29.5) | 364 (61.8) | 51 (8.7) | <0.001 |
| Dairy | 7 (1.4) | 129 (26.1) | 359 (72.5) | 14 (2.4) | 167 (28.2) | 410 (69.4) | 0.35 |
| Soft drinks | 44 (8.9) | 308 (62.2) | 143 (28.9) | 123 (20.8) | 350 (59.1) | 119 (20.1) | <0.001 |
| Pastries | 42 (8.5) | 379 (76.9) | 72 (14.6) | 83 (14.1) | 447 (75.6) | 61 (10.3) | 0.004 |
| Sweets | 161 (32.9) | 293 (59.8) | 36 (7.3) | 182 (30.9) | 363 (61.6) | 44 (7.5) | 0.79 |
| Milk desserts | 81 (16.5) | 307 (62.4) | 104 (21.1) | 181 (30.6) | 336 (56.9) | 74 (12.5) | <0.001 |
| Crisps | 66 (13.4) | 380 (77.1) | 47 (9.5) | 101 (17.1) | 455 (77.0) | 35 (5.9) | 0.03 |
| Sausages | 18 (3.6) | 352 (71.3) | 124 (25.1) | 36 (6.1) | 408 (69.2) | 146 (24.7) | 0.18 |
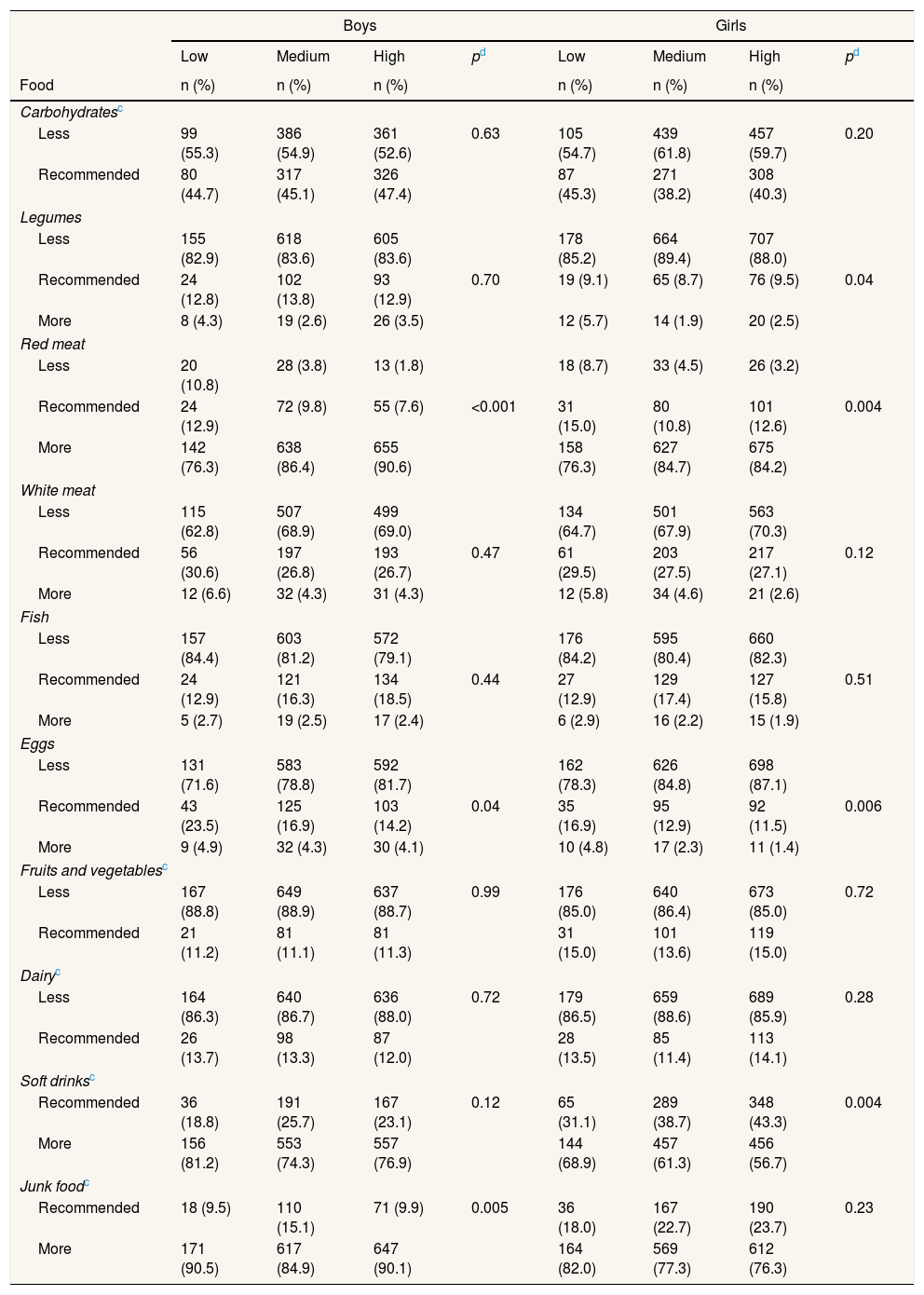
Regarding eating red meat, boys and girls in the lowest FAS level showed the highest prevalence of complying with food recommendations (12% in boys and 15% in girls) compared to the adolescents in the medium FAS (9.8% and 10.8%, respectively) and the highest FAS (7.6% and 12.6%). Furthermore, adolescents in the highest FAS showed a higher prevalence of eating red meat “more than recommended” (90.6% in boys and 84.2% in girls) than adolescents in the lowest FAS (76.3% in both sexes). Moreover, egg consumption in boys followed an SES gradient, with students from the lowest FAS being those who had the highest prevalence of complying with food recommendations (23.5%) compared with the medium (16.9%) and highest (14.2%) FAS. As for the recommended frequency of soft drinks, significant differences were observed among girls by FAS. Girls from the highest FAS had a higher prevalence of complying with the soft drink recommendations than girls in the lowest FAS (43.3% and 31.1% respectively) (p=0.004) (Table 4).
| Boys | Girls | |||||||
|---|---|---|---|---|---|---|---|---|
| Low | Medium | High | pd | Low | Medium | High | pd | |
| Food | n (%) | n (%) | n (%) | n (%) | n (%) | n (%) | ||
| Carbohydratesc | ||||||||
| Less | 99 (55.3) | 386 (54.9) | 361 (52.6) | 0.63 | 105 (54.7) | 439 (61.8) | 457 (59.7) | 0.20 |
| Recommended | 80 (44.7) | 317 (45.1) | 326 (47.4) | 87 (45.3) | 271 (38.2) | 308 (40.3) | ||
| Legumes | ||||||||
| Less | 155 (82.9) | 618 (83.6) | 605 (83.6) | 178 (85.2) | 664 (89.4) | 707 (88.0) | ||
| Recommended | 24 (12.8) | 102 (13.8) | 93 (12.9) | 0.70 | 19 (9.1) | 65 (8.7) | 76 (9.5) | 0.04 |
| More | 8 (4.3) | 19 (2.6) | 26 (3.5) | 12 (5.7) | 14 (1.9) | 20 (2.5) | ||
| Red meat | ||||||||
| Less | 20 (10.8) | 28 (3.8) | 13 (1.8) | 18 (8.7) | 33 (4.5) | 26 (3.2) | ||
| Recommended | 24 (12.9) | 72 (9.8) | 55 (7.6) | <0.001 | 31 (15.0) | 80 (10.8) | 101 (12.6) | 0.004 |
| More | 142 (76.3) | 638 (86.4) | 655 (90.6) | 158 (76.3) | 627 (84.7) | 675 (84.2) | ||
| White meat | ||||||||
| Less | 115 (62.8) | 507 (68.9) | 499 (69.0) | 134 (64.7) | 501 (67.9) | 563 (70.3) | ||
| Recommended | 56 (30.6) | 197 (26.8) | 193 (26.7) | 0.47 | 61 (29.5) | 203 (27.5) | 217 (27.1) | 0.12 |
| More | 12 (6.6) | 32 (4.3) | 31 (4.3) | 12 (5.8) | 34 (4.6) | 21 (2.6) | ||
| Fish | ||||||||
| Less | 157 (84.4) | 603 (81.2) | 572 (79.1) | 176 (84.2) | 595 (80.4) | 660 (82.3) | ||
| Recommended | 24 (12.9) | 121 (16.3) | 134 (18.5) | 0.44 | 27 (12.9) | 129 (17.4) | 127 (15.8) | 0.51 |
| More | 5 (2.7) | 19 (2.5) | 17 (2.4) | 6 (2.9) | 16 (2.2) | 15 (1.9) | ||
| Eggs | ||||||||
| Less | 131 (71.6) | 583 (78.8) | 592 (81.7) | 162 (78.3) | 626 (84.8) | 698 (87.1) | ||
| Recommended | 43 (23.5) | 125 (16.9) | 103 (14.2) | 0.04 | 35 (16.9) | 95 (12.9) | 92 (11.5) | 0.006 |
| More | 9 (4.9) | 32 (4.3) | 30 (4.1) | 10 (4.8) | 17 (2.3) | 11 (1.4) | ||
| Fruits and vegetablesc | ||||||||
| Less | 167 (88.8) | 649 (88.9) | 637 (88.7) | 0.99 | 176 (85.0) | 640 (86.4) | 673 (85.0) | 0.72 |
| Recommended | 21 (11.2) | 81 (11.1) | 81 (11.3) | 31 (15.0) | 101 (13.6) | 119 (15.0) | ||
| Dairyc | ||||||||
| Less | 164 (86.3) | 640 (86.7) | 636 (88.0) | 0.72 | 179 (86.5) | 659 (88.6) | 689 (85.9) | 0.28 |
| Recommended | 26 (13.7) | 98 (13.3) | 87 (12.0) | 28 (13.5) | 85 (11.4) | 113 (14.1) | ||
| Soft drinksc | ||||||||
| Recommended | 36 (18.8) | 191 (25.7) | 167 (23.1) | 0.12 | 65 (31.1) | 289 (38.7) | 348 (43.3) | 0.004 |
| More | 156 (81.2) | 553 (74.3) | 557 (76.9) | 144 (68.9) | 457 (61.3) | 456 (56.7) | ||
| Junk foodc | ||||||||
| Recommended | 18 (9.5) | 110 (15.1) | 71 (9.9) | 0.005 | 36 (18.0) | 167 (22.7) | 190 (23.7) | 0.23 |
| More | 171 (90.5) | 617 (84.9) | 647 (90.1) | 164 (82.0) | 569 (77.3) | 612 (76.3) | ||
“Carbohydrates”, “fruits and vegetables” and “dairies” are recommended to be eaten every day. Therefore, the categories possible according to the question in the questionnaire were “recommended” or “less than recommended”. “Soft drinks” and “junk food” are recommended to be eaten occasionally. Therefore, the possible categories are “recommended” or “more than recommended”.
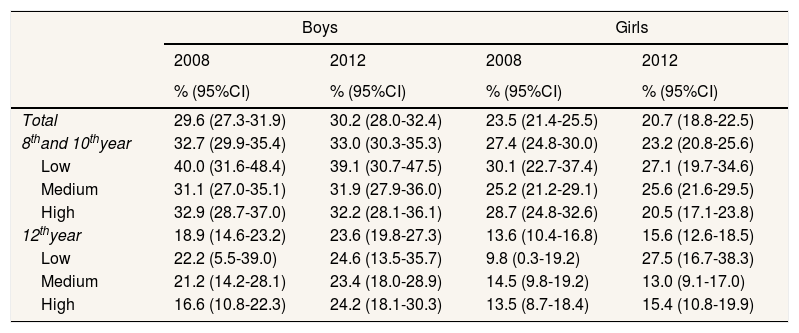
According to the WHO cut-off points, differences in the prevalences of excess weight between 2008 and 2012 were found among girls in the 8th and 10th decreasing from 28.7% (95%CI: 24.8-32.6) to 20.5% (95%CI: 17.1-23.8) in girls in the highest FAS (Table 5).
| Boys | Girls | |||
|---|---|---|---|---|
| 2008 | 2012 | 2008 | 2012 | |
| % (95%CI) | % (95%CI) | % (95%CI) | % (95%CI) | |
| Total | 29.6 (27.3-31.9) | 30.2 (28.0-32.4) | 23.5 (21.4-25.5) | 20.7 (18.8-22.5) |
| 8thand 10thyear | 32.7 (29.9-35.4) | 33.0 (30.3-35.3) | 27.4 (24.8-30.0) | 23.2 (20.8-25.6) |
| Low | 40.0 (31.6-48.4) | 39.1 (30.7-47.5) | 30.1 (22.7-37.4) | 27.1 (19.7-34.6) |
| Medium | 31.1 (27.0-35.1) | 31.9 (27.9-36.0) | 25.2 (21.2-29.1) | 25.6 (21.6-29.5) |
| High | 32.9 (28.7-37.0) | 32.2 (28.1-36.1) | 28.7 (24.8-32.6) | 20.5 (17.1-23.8) |
| 12thyear | 18.9 (14.6-23.2) | 23.6 (19.8-27.3) | 13.6 (10.4-16.8) | 15.6 (12.6-18.5) |
| Low | 22.2 (5.5-39.0) | 24.6 (13.5-35.7) | 9.8 (0.3-19.2) | 27.5 (16.7-38.3) |
| Medium | 21.2 (14.2-28.1) | 23.4 (18.0-28.9) | 14.5 (9.8-19.2) | 13.0 (9.1-17.0) |
| High | 16.6 (10.8-22.3) | 24.2 (18.1-30.3) | 13.5 (8.7-18.4) | 15.4 (10.8-19.9) |
95%CI: 95% confidence interval.
Food frequency differences in the economic crisis were observed between boys and girls, with girls eating fruits and vegetables more frequently. In addition, less than a half of the adolescents were currently following the recommendations of the “food recommendation pyramid”. Finally, excess weight is higher in boys than in girls, and decreased in girls from the highest SES and in the 8th to 10th years of education between 2008 and 2012.
The results of this study, showing that girls ate more fruit and vegetables than boys, are concordant with those in previous studies conducted in Madrid and the Balearic Islands21,22 as well as in other European studies.23 The results on food consumption in boys were also consistent with the SIVFRENT report, showing that adolescents in Madrid ate bread, crisps and biscuits in a higher frequency than girls.
The prevalence of compliance with food recommendations among adolescents was lower than 50%, independently of SES. Most adolescents consume more junk food, soft drinks and red meat than recommended and eat fewer fruits and vegetables than recommended, as described in other studies.21,23,24 In this regard, it is important that the “food recommendation pyramid” used in this study was based on the Mediterranean diet, while some studies report a shift towards more westernised diets and an abandonment of the Mediterranean diet, which could partially explain the results found in our study.
Differences in consumption by SES were not found for most of the types of food analysed, although red meat, eggs, junk food and soft drinks showed an SES gradient. It is well documented that people from lower SES groups consume more junk food than those from higher SES groups,25 as indicated by our results. With reference to meat and eggs, Tatiana Andrayeva et al. pointed out that in the USA the demand for meat (especially beef) is related to the cost of the product (elastic demand) but the demand of eggs is not (inelastic demand).26 Additionally, these authors concluded that increasing food prices or reducing family incomes may influence family food purchasing. Indeed, a study with a representative sample of the Finnish population aimed to explore if the reasons of the food choice were related to income and education. Finnish with low SES reported that price and income were the main motivations in food purchasing decisions compared to those in the highest SES groups who prioritize healthy food.27 In our study, adolescents in the lowest FAS less frequently ate red meat and more often ate eggs than adolescents in the highest FAS, which could be explained by economic factors such as family income, which may influence the shopping basket. In contrast, no differences in fruit and vegetable consumption were observed by SES. Although it is generally believed that fruit and vegetable consumption follows an SES gradient,26–28 the results of this study are concordant with the theory that the SES gradient depends on the availability/affordability of these products. In southern European countries, such as Spain, fruit and vegetables are widely available and affordable, so their consumption is not strongly associated with SES, as is sometimes the case in northern European countries.29,30 Although the study design does not allow us to attribute differences between SES in the eating frequencies to the economic crisis, these results are consistent with those reported in the SESPAS report.31 Furthermore, some authors suggest that SES differences can be found in the variety and quality of the fruits consumed rather than in the quantity.32
The prevalence of excess weight in boys was higher than in girls. These results confirm the findings observed in previous studies describing the same pattern.1,33,34 When 2008 and 2012 were compared, excess weight differences were only found among girls from the highest SES, showing a decrease in the prevalence. Different tendencies in excess weight in Spain have been observed depending on the definition taken.1 Some tendencies show that excess weight is still increasing,1 but others suggest that it has reached a plateau and even has decreased in girls.35 The excess weight reduction among girls, especially in those in the 8th to 10th years in the highest SES, indicates that socioeconomic inequalities in excess weight among girls could be increasing in Barcelona.
This study has some limitations. Firstly, the study might be affected by information bias due to the use of self-reported questionnaires. However, the questionnaire was anonymous and eating habits are not a sensitive topic, so this bias is not expected to be relevant. Secondly, the FRESC survey is a generalist questionnaire, which was not exclusively designed to study eating habits. However, the questions on this topic were designed in concordance with the “food recommendation pyramid” and belonged to other food frequency questionnaires. In addition, the questionnaire has not been previously validated. Nevertheless, self-administered food frequency questionnaires for adolescents are a common tool in epidemiological studies and previous studies have shown that anonymous self-reported food frequency questionnaires have fair to moderate validity.36 Finally, it was not possible to compare the food consumption between 2008 and 2012, since, unfortunately, the questionnaires differed from each other between FRESC editions.
One of the strengths of our study is that studies showing details on food consumption frequency in adolescents in an economic crisis context are scarce. Therefore, the results of this study provide the first data on this important topic. The sample used was representative of adolescents in Barcelona. Furthermore, both 2008 and 2012 FRESC surveys gathers objective information on height and weight. Consequently, comparison between 2008 and 2012 editions was possible.
This study observed a low prevalence of adolescents following food recommendations, as well as differences between sex in the food frequency consumption, even in an economic crisis. Importantly, excess weight was higher in boys than in girls, and SES differences between 2008 and 2012 among girls have been observed. Further studies should be conducted to monitor the eating habits of adolescents and meeting the food recommendations and to detect the key associated factors. According to our results, health promotion programs including a gender perspective seem to be needed to improve eating habits among adolescents. In addition, results on differences in excess weight related to adolescents’ SES clearly support the need of public policies focused on reducing social inequalities.
Editor in chargeM. Felicitas Domínguez Berjón.
The prevalence of excess weight in adolescents is high, and good eating habits are especially important due to the physical and mental development that takes place at this stage. The economic crisis might affect the eating habits of adolescents in Spain.
What does this study add to the literature?Less than 50% of adolescents meet food recommendations and socioeconomic differences were found. Excess weigh decreased between 2008 and 2012 in girls from the highest socioeconomic position. There is a need to promote programs and policies to reduce socioeconomic and sex inequalities related to eating habits and excess weight in adolescents.
X. Continente, M.J. López and A. Pérez-Giménez designed and conducted the study. T. Arechavala-Roe analyzed the data and drafted the manuscript. X. Continente and M.J. López supervised the document, helped to interpret data and made further suggestions. Finally, A. Pérez-Giménez, F. Sánchez-Martínez and X. Bartoll helped to interpret data and critically revised the document. All authors approved the final manuscript as submitted.
FundingThis work was partially supported by the Agència de Gestió d’Ajuts Universitaris i de Recerca de la Generalitat de Catalunya (AGAUR SGR 2009-1345).
Conflicts of interestOne of the authors (M.J.L.) belongs to the Gaceta Sanitaria editorial committee, but was not involved in the editorial process of the manuscript.
The authors would like to thank teachers and students for participating in this study. We would also like to thank the “community health service” and the “evaluation methods and intervention service” of the ASPB for their help in administering the questionnaire, taking weight and height measurements and creating the database.











