



To determine the prevalence of negative mood states in adolescents according to gender, to analyze variability among schools, and to evaluate the associated factors.
MethodsA cross-sectional study with a cluster design was carried out. We administered the High-school students health survey to a sample of 9,340 students (aged 14-16 years) in the third and fourth year of Compulsory Secondary Education in Catalonia, Spain, during the 2005-6 academic year. The main outcome measure was evidence of a negative mood state. A multilevel logistic regression model stratified by gender was used to identify the factors associated with negative mood states and to determine variability among distinct schools.
ResultsApproximately 19% of adolescents reported evidence of a negative mood state, with a higher prevalence in girls (25%). The most significant factors associated with negative mood states were “use of tranquilizers” and “having eating disorders” in girls and “not exercising” and “poor self-perception of health status” in boys. In both genders, variability was found among schools in the prevalence of negative mood states (girls: variance = 0.078; p <0.001; boys: variance = 0.079; p = 0.012).
ConclusionsThe prevalence of negative mood states in adolescent boys and girls was high. Differences were observed between genders in the factors related to these health states. The variability observed in the prevalence of negative mood states among distinct schools could not be explained by the study variables. Our results emphasize the association between the use of tranquilizers and negative mood states.
Determinar la prevalencia del estado de ánimo negativo entre alumnos adolescentes según sexo, analizar la variabilidad entre escuelas y evaluar los factores asociados.
MétodosEstudio transversal basado en un muestreo por conglomerados bietápico. Administramos una encuesta de salud a 9340 estudiantes de tercero y cuarto curso de Educación Secundaria Obligatoria de 14 a 16 años de edad, en Cataluña, durante el curso escolar 2005-06. La variable principal fue el estado de ánimo negativo. Se usó un modelo de regresión logística multinivel estratificado por sexo para identificar los factores asociados al estado de ánimo negativo y determinar la variabilidad entre las diferentes escuelas.
ResultadosAproximadamente el 19% de los adolescentes refirieron un estado de ánimo negativo, siendo más prevalente entre las chicas (25%). En ellas, los factores asociados significativamente con estados de ánimo negativo fueron «tomar tranquilizantes» y tener trastornos alimentarios, mientras que en los chicos fueron no realizar deporte y tener una mala percepción de su estado de salud. Hay variabilidad en la prevalencia del estado de ánimo negativo según las escuelas en ambos sexos (chicas: varianza = 0,078, p <0,001; chicos: varianza = 0,079, p = 0,012).
ConclusionesLa prevalencia del estado de ánimo negativo entre los adolescentes fue alta. Se observaron diferencias entre sexos respecto a los factores relacionados con este estado de salud. Destacó la asociación del uso de tranquilizantes con el estado de ánimo negativo. Se observó una variabilidad de la prevalencia del estado de ánimo negativo entre las diferentes escuelas no explicada por las variables de estudio.
Mental disorders that are seen in adults often begin during adolescence1 and the many transformations currently occurring in family, community and societal values, functions and structures increase the complexity of the environment faced by adolescents. According to the World Health Organization, 20% of adolescents suffer from mental health problems, and by the year 2020, childhood and adolescent mental health problems will become one of the leading causes of morbidity, mortality and disability among children worldwide.2 Depressive disorders are common during adolescence,2 and depressive symptomatology is frequently undiagnosed and is especially undertreated in adolescents.2,3
Numerous studies have addressed depressive symptomatology in adolescents. Some of these analyze its association with risk factors such as substance abuse, risky sexual practices, eating disorders, bullying and antisocial behavior.3–6 Other studies identify gender as an associated factor.7,8 However, few studies have assessed the complexity of all of these associated factors as a whole or the influence of gender on these causal relationships.4,8 In addition, although most researchers have studied adolescents who attend school they have generally not taken into account the group factors that might influence individual mood. Ahonen et al8 did suggest that the school in which a student studies could influence mood states and related factors.
Early recognition of depressive symptomatology is important to reduce the prevalence of depression among older individuals.3 Symptoms such as sadness, hopelessness or boredom reflect a negative mood state that can precede a more severe affective disorder. For these reasons, mood states in adolescents and factors related to these states should be explored by gender. Furthermore, optimal awareness of adolescent mood states and the associated risk factors is important to allow interventions in school situations against preventable risk factors.
In this context, the implementation of the “Health and School” (Salut i Escola)9 program during the 2005-6 academic year, in the third and fourth year of Compulsory Secondary Education (CSE), in Catalonia (Spain), allowed the habits and behaviors related to adolescent health, including mood states and related factors, to be studied.
The present study sought to examine the prevalence of negative mood states (i.e., the presence of symptoms associated with depression such as boredom, hopelessness, sadness, nervousness and difficulty sleeping) in adolescents between the ages of 14 and 16, and to identify the possible factors associated with these states by gender, through a school survey. A further aim was to assess and quantify variation in negative mood states among schools, and to evaluate the factors that could account for any differences found.
MethodsWe used data from the “High school students health survey” administered from February to June during the 2005-06 academic year, to third- and fourth-year CSE students, between 14 and 16 years of age in Catalonia, Spain.
The 94-item questionnaire was paper-based and self-administered, based on a questionnaire designed by the Barcelona Public Health Agency “Risk Factors Among School Age Children”,10 a group of experts from the Department of Health, and a review of literature,11 as well as other national12–14 and international questionnaires.15,16
A two-stage sample was performed. In the first stage, the primary sampling unit was the school, previously stratified by health region by non-proportional sampling and within the region by funding type (public or private). The health regions are determined by the Catalan Health Service.17 In the second stage, three classes were randomly selected in each school and all students from the third and fourth year of these classes were included. In schools with fewer than three classes, all classes were selected.
The sample size was calculated based on a sampling frame of 978 schools, with an estimated enrolment of 125,389 students (according to data available from the school academic year 2004-2005) and independently in each of the strata. Given the cluster design, we assumed an intraclass correlation coefficient (ICC) of 0.02,18,19 the average number of students per school per health region, a 50% event rate, an two-tailed alpha significance level of 0.07 in the small health regions, a two-tailed alpha of 0.05 in the other health regions, and a statistical power of 80%. We oversampled certain regions to enhance the precision of the population estimates and then performed a subgroup analysis by health region. To reduce the effect of possible non-participation of some of the schools selected, the sample size was increased by 20%.
Finally, 111 schools (13,165 eligible students) were selected. Questionnaires were returned by 97 schools and 9,340 students, a 71% response rate representing 7,35% of the 127,010 students in this age group in Catalonia. Study results were reported to the directors of the selected schools and to the respective associations of students’ parents. The questionnaires were administered in groups in the presence of an expert trained researcher and without the presence of a school tutor or teacher.
Evidence of a negative mood state was our response variable, which contained the following items adapted from other studies8,10,20: how many times have you felt: very tired doing normal activities?; out of place, sad or depressed?; hopeless facing the future?; nervous or tense?; bored with things?; threatened by another student at school?; or had difficulty sleeping or staying asleep? Answers were collected on a five-option Likert scale ranging from “never” to “always”.
To differentiate occasional experiences or the experience of possibly problematic negative mood states, we created a dichotomous variable. Answers were divided into two categories, where “never”, “almost never”, or “sometimes” constituted one group (0 points), and “frequently” or “always” constituted the other group (1 point). Students who accumulated three or more points were considered to have negative mood states.
The covariates considered were the following sociodemographic and general variables: year in school (third or fourth year of CSE), considered as a proxy for age since the program includes actions and interventions directed at each grade; gender (male/female); student's country of origin (foreigner if not born in Spain/non-foreigner); living with both parents (yes/no); parents unemployed (yes/no); self-perception of academic achievement (high, medium or low); and self-perception of general health (excellent, very good, good, normal or poor), dichotomized as good/poor; physical activity (never, sometimes or every day). To assess the risk of eating disorders, the Spanish validated version of the Sick, Control, One Fat, Food (SCOFF)14 questionnaire was used. Students with two or more affirmative answers were considered at risk of having an eating disorder (yes/no).
The following variables related to the use of substances were considered as dichotomous covariates (yes/no): use of tobacco in the last 30 days; alcoholic drink in the last 30 days; being drunk in the last 6 months; use of tranquilizers, whether as sleeping pills or for nerves; use of cannabis; use of cocaine; use of amphetamines; driving under the effects of alcohol or drugs; and riding in a car with a driver who was under the effects of alcohol or drugs. Opinions on the use of cannabis, tranquilizers and other drugs were categorized as dangerous/not dangerous.
A group of variables related to behavior was assessed (anti-social behaviors, bullying, violence, abuse, sexual activity): anti-social behaviors included a positive answer to skipping school one or more times, fighting, breaking or stealing things, playing to win money; experience with bullying included the experience of being laughed at, insulted, hit, attacked or threatened, teased or marginalized twice or more in the last 12 months; participating in bullying included laughing at, insulting, hit, attacking or threatening other students, teasing or marginalizing other students; violent behaviour was indicated by a positive answer (yes/no) to either fighting outside or in school twice or more in the past 12 months, or to having required medical attention after a fight at some time in the same time period. Variables related to abuse included perceived physical abuse, perceived psychological abuse, and perceived sexual abuse (yes/no). Sexual behavior was assessed by one question: sexual relations with penetration (yes/no).
School-level covariates included the type of school according to funding (private/public).
Statistical analysisWe performed a stratified analysis according to gender. Data were weighted to take into account the design effect inherent in the use of multistage cluster sampling, as well as to ensure that the sample would be representative of the student population in Catalonia. Descriptive results are presented as weighted proportions and unweighted number of students.
We applied multilevel statistical procedures21,22 to investigate the effect of individual student factors on having a negative mood state, as well as to investigate the extent to which the school might account for any variations in the outcome. We used the binomial logit link with full maximum likelihood method of estimation via the iterative Laplace algorithm approximation.
We modeled students (level-1 units) as nested within 97 schools (level-2 units).
Initially, we examined whether there were differences in having a negative mood state among schools by fitting an unconditional model, i.e., with no covariates at either level. The second model estimated the effect of student-level covariates on the outcome and determined whether these effects varied by school (i.e. allowing for level-2 random effects). Finally, we added school-level covariates to the previous model to determine whether school variation could be accounted for by these contextual factors.
All statistical tests were two-sided at the 5% significance level. The analyses were carried out using the HLM for Windows multilevel package, version 10.1 and Stata/SE version 9.1(Stata Corp.).
ResultsThe final sample from the high school students’ health survey data was comprised of 9,340 students, including 4,687 (50.1%) girls, 51.8% of whom were third-year students. The mean age was 15 years (range: 14-18).
After removing an incoherent item (“being threatened by another student at school”) from the construct, Cronbach's alpha for the mood states indicator was 0.767 for boys, and 0.773 for girls.
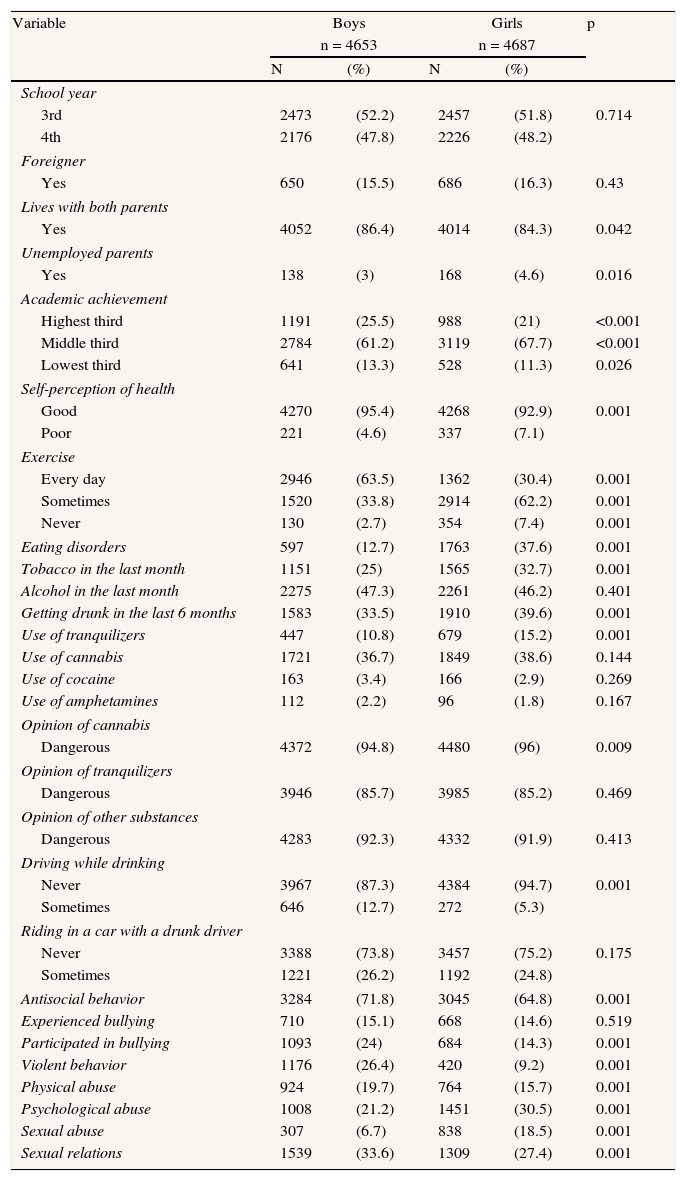
Boys reported higher levels of academic achievement and health, and more frequently claimed to exercise daily, while in girls a greater risk of having an eating disorder (SCOFF) was observed (almost three times more than in boys).
A greater use of tobacco in the last month, more episodes of drunkenness in the last 6 months, and greater use of tranquilizers was observed in girls. Antisocial behavior, violent behavior and participation in bullying were more prevalent in boys.
Girls expressed more emotional and sexual abuse, while boys reported more physical abuse and sexual relations (Table 1).
General characteristics of the sample. Health and School survey.
| Variable | Boys | Girls | p | ||
| n = 4653 | n = 4687 | ||||
| N | (%) | N | (%) | ||
| School year | |||||
| 3rd | 2473 | (52.2) | 2457 | (51.8) | 0.714 |
| 4th | 2176 | (47.8) | 2226 | (48.2) | |
| Foreigner | |||||
| Yes | 650 | (15.5) | 686 | (16.3) | 0.43 |
| Lives with both parents | |||||
| Yes | 4052 | (86.4) | 4014 | (84.3) | 0.042 |
| Unemployed parents | |||||
| Yes | 138 | (3) | 168 | (4.6) | 0.016 |
| Academic achievement | |||||
| Highest third | 1191 | (25.5) | 988 | (21) | <0.001 |
| Middle third | 2784 | (61.2) | 3119 | (67.7) | <0.001 |
| Lowest third | 641 | (13.3) | 528 | (11.3) | 0.026 |
| Self-perception of health | |||||
| Good | 4270 | (95.4) | 4268 | (92.9) | 0.001 |
| Poor | 221 | (4.6) | 337 | (7.1) | |
| Exercise | |||||
| Every day | 2946 | (63.5) | 1362 | (30.4) | 0.001 |
| Sometimes | 1520 | (33.8) | 2914 | (62.2) | 0.001 |
| Never | 130 | (2.7) | 354 | (7.4) | 0.001 |
| Eating disorders | 597 | (12.7) | 1763 | (37.6) | 0.001 |
| Tobacco in the last month | 1151 | (25) | 1565 | (32.7) | 0.001 |
| Alcohol in the last month | 2275 | (47.3) | 2261 | (46.2) | 0.401 |
| Getting drunk in the last 6 months | 1583 | (33.5) | 1910 | (39.6) | 0.001 |
| Use of tranquilizers | 447 | (10.8) | 679 | (15.2) | 0.001 |
| Use of cannabis | 1721 | (36.7) | 1849 | (38.6) | 0.144 |
| Use of cocaine | 163 | (3.4) | 166 | (2.9) | 0.269 |
| Use of amphetamines | 112 | (2.2) | 96 | (1.8) | 0.167 |
| Opinion of cannabis | |||||
| Dangerous | 4372 | (94.8) | 4480 | (96) | 0.009 |
| Opinion of tranquilizers | |||||
| Dangerous | 3946 | (85.7) | 3985 | (85.2) | 0.469 |
| Opinion of other substances | |||||
| Dangerous | 4283 | (92.3) | 4332 | (91.9) | 0.413 |
| Driving while drinking | |||||
| Never | 3967 | (87.3) | 4384 | (94.7) | 0.001 |
| Sometimes | 646 | (12.7) | 272 | (5.3) | |
| Riding in a car with a drunk driver | |||||
| Never | 3388 | (73.8) | 3457 | (75.2) | 0.175 |
| Sometimes | 1221 | (26.2) | 1192 | (24.8) | |
| Antisocial behavior | 3284 | (71.8) | 3045 | (64.8) | 0.001 |
| Experienced bullying | 710 | (15.1) | 668 | (14.6) | 0.519 |
| Participated in bullying | 1093 | (24) | 684 | (14.3) | 0.001 |
| Violent behavior | 1176 | (26.4) | 420 | (9.2) | 0.001 |
| Physical abuse | 924 | (19.7) | 764 | (15.7) | 0.001 |
| Psychological abuse | 1008 | (21.2) | 1451 | (30.5) | 0.001 |
| Sexual abuse | 307 | (6.7) | 838 | (18.5) | 0.001 |
| Sexual relations | 1539 | (33.6) | 1309 | (27.4) | 0.001 |
Percentages are weighted proportions.
The p-values were calculated using the weighted Chi-squared test, with comparison between genders.
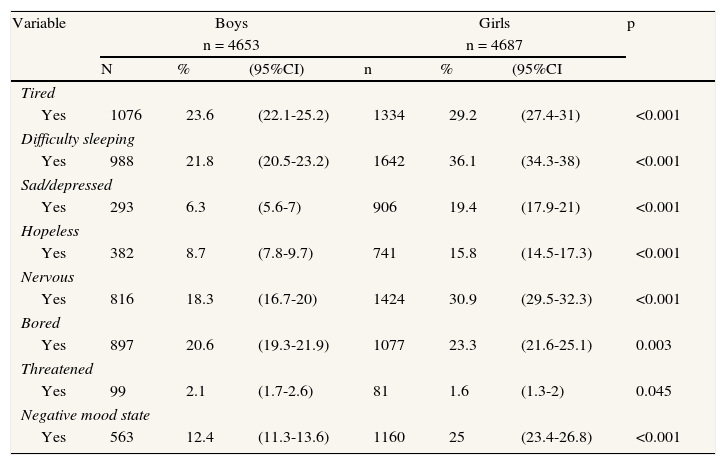
Approximately 19% (95%CI: 17.6%–19.9%) of the sample population reported evidence of a negative mood state, with a higher prevalence in girls (25%, more than twice that of boys). All of the response variable items were more prevalent in girls, except for “feeling threatened by another student at school”. Remarkably, sadness or depression was more than three times more prevalent in girls and hopelessness was almost double. The item most frequently reported in girls was “difficulty sleeping”, while that most frequently reported in boys was tiredness.
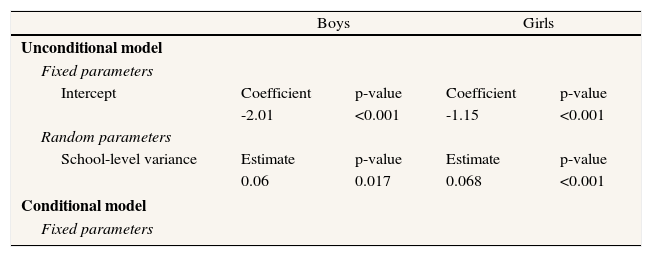
The model with no covariates at either level (the unconditional model) showed that the expected prevalence of girls with a negative mood state was 24% with a magnitude of variation among schools of 15.9% to 34.6%. In boys, the expected prevalence was 11.8% with a range of variation among schools of 7.6% to 17.8%. This model revealed that a relatively small percentage of the total individual variability in having a negative mood state was attributable to the school level (ICC = 2.3%) (Table 2).
Frequency of negative mood states by item and by gender. Health and School survey.
| Variable | Boys | Girls | p | ||||
| n = 4653 | n = 4687 | ||||||
| N | % | (95%CI) | n | % | (95%CI | ||
| Tired | |||||||
| Yes | 1076 | 23.6 | (22.1-25.2) | 1334 | 29.2 | (27.4-31) | <0.001 |
| Difficulty sleeping | |||||||
| Yes | 988 | 21.8 | (20.5-23.2) | 1642 | 36.1 | (34.3-38) | <0.001 |
| Sad/depressed | |||||||
| Yes | 293 | 6.3 | (5.6-7) | 906 | 19.4 | (17.9-21) | <0.001 |
| Hopeless | |||||||
| Yes | 382 | 8.7 | (7.8-9.7) | 741 | 15.8 | (14.5-17.3) | <0.001 |
| Nervous | |||||||
| Yes | 816 | 18.3 | (16.7-20) | 1424 | 30.9 | (29.5-32.3) | <0.001 |
| Bored | |||||||
| Yes | 897 | 20.6 | (19.3-21.9) | 1077 | 23.3 | (21.6-25.1) | 0.003 |
| Threatened | |||||||
| Yes | 99 | 2.1 | (1.7-2.6) | 81 | 1.6 | (1.3-2) | 0.045 |
| Negative mood state | |||||||
| Yes | 563 | 12.4 | (11.3-13.6) | 1160 | 25 | (23.4-26.8) | <0.001 |
Percentages are weighted proportions.
The p-values were calculated using the weighted Chi-squared test, with comparison between genders.
On average, regardless of gender, the factors that were positively associated with the probability of having a negative mood state were “use of tranquilizers”, “having an eating disorder” and “perceived psychological mistreatment”. These factors were of similar magnitude in both genders, and students displaying these factors were more than twice as likely to report evidence of a negative mood state.
In girls, the most significant factors associated with negative mood states were “use of tranquilizers” and “having an eating disorder”, while in boys these factors were “no exercise” and “poor self-perception of health status”.
Girls who had medium or low self-perception of academic performance, those who reported sexual abuse, and those who had used tobacco and alcohol were more likely to report negative mood states. These associations were not found in boys.
There were no gender-based differences between other factors that were positively associated with the probability of reporting a negative mood state.
After accounting for student and school characteristics, there was a statistically significant difference among schools in the prevalence of negative mood states in both genders (girls: variance = 0.078, p <0.001; boys: variance = 0.079, p = 0.012) (Table 3).
Factors associated with the odds of having a negative mood state by gender. Multilevel logistic regression.
| Boys | Girls | |||
| Unconditional model | ||||
| Fixed parameters | ||||
| Intercept | Coefficient | p-value | Coefficient | p-value |
| -2.01 | <0.001 | -1.15 | <0.001 | |
| Random parameters | ||||
| School-level variance | Estimate | p-value | Estimate | p-value |
| 0.06 | 0.017 | 0.068 | <0.001 | |
| Conditional model | ||||
| Fixed parameters | ||||
| Unadjusted | Adjusteda | Unadjusted | Adjusteda | |||||
| OR | (CI) | OR | (CI) | OR | (CI) | OR | (CI) | |
| Academic achievement | ||||||||
| Highest third | 3.38 | (2.70-4.22) | 2.14 | (1.59-2.88) | ||||
| Middle third | 1.49 | (1.23- 1.81) | 1.28 | (1.01-1.62) | ||||
| Lowest third | 1 | 1 | ||||||
| Self-perception of health | ||||||||
| Poor | 4.25 | (3.24-5.57) | 2.40 | (1.71-3.38) | 3.62 | (2.87-4.57) | 1.77 | (1.27-2.46) |
| Good | 1 | 1 | 1 | 1 | ||||
| Exercise | ||||||||
| Never | 3.80 | (2.43-5.93) | 2.52 | (1.48-4.29) | 2.02 | (1.58-2.58) | 1.87 | (1.33-2.62) |
| Sometimes | 1.56 | (1.31-1.86) | 1.26 | (1.03-1.54) | 1.45 | (1.11-1.57) | 1.19 | (0.96-1.47) |
| Every day | 1 | 1 | 1 | 1 | ||||
| Eating disorders | ||||||||
| Yes | 2.98 | (2.42-3.67) | 2.03 | (1.62-2.55) | 3.08 | (2.71-3.51) | 2.29 | (1.88-2.79) |
| No | 1 | 1 | 1 | 1 | ||||
| Tobacco in the last month | ||||||||
| Yes | 1.87 | (1.61-2.16) | 1.17 | (0.95-1.45) | ||||
| No | 1 | 1 | ||||||
| Alcohol in the last month | ||||||||
| Yes | 1.56 | (1.37-1.78) | 1.23 | (1.01-1.51) | ||||
| No | 1 | 1 | ||||||
| Getting drunk in the last 6 months | ||||||||
| Yes | 1.48 | (1.30-1.69) | 0.79 | (0.64-0.97) | ||||
| No | 1 | 1 | ||||||
| Use of tranquilizers | ||||||||
| Yes | 3.39 | (2.70-4.25) | 2.31 | (1.76-3.03) | 3.54 | (2.96-4.22) | 2.67 | (2.08-3.43) |
| No | 1 | 1 | 1 | 1 | ||||
| Opinion of cannabis | ||||||||
| Not dangerous | 2.08 | (1.48-2.92) | 1.48^ | (0.98-2.24) | 1.76 | (1.28-2.44) | 1.52b | (0.98-2.36) |
| Dangerous | 1 | 1 | 1 | 1 | ||||
| Antisocial behavior | ||||||||
| Yes | 2.57 | (2.07-3.18) | 1.68 | (1.33-2.13) | 2.45 | (2.10-2.87) | 1.52 | (1.24-1.86) |
| No | 1 | 1 | 1 | 1 | ||||
| Experienced bullying | ||||||||
| Yes | 2.84 | (2.34-3.44) | 1.53 | (1.20-1.96) | 2.43 | (2.03-2.91) | 1.56 | (1.25-1.94) |
| No | 1 | 1 | 1 | 1 | ||||
| Participated in bullying | ||||||||
| Yes | 2.09 | (1.78-2.44) | 1.41 | (1.16-1.73) | 2.006 | (1.67-2.41) | 1.32 | (1.06-1.64) |
| No | 1 | 1 | 1 | 1 | ||||
| Psychological abuse | ||||||||
| Yes | 3.39 | (2.83-4.06) | 2.35 | (1.90-2.91) | 3.48 | (3.07-3.95) | 2.21 | (1.88-2.61) |
| No | 1 | 1 | 1 | 1 | ||||
| Sexual abuse | ||||||||
| Yes | 2.54 | (2.17-2.98) | 1.85 | (1.47-2.33) | ||||
| No | 1 | 1 | ||||||
| Random parameters | ||||||||
| school-level variance | Estimate | p-value | Estimate | p-value | ||||
| 0.079 | 0.012 | 0.078 | <0.001 | |||||
OR: odds ratio; CI: confidence interval.
Unadjusted: crude OR from separate univariate logistic models.
Adjusted: ORs further adjusted by the remaining variables presented in the table.
The most important result of the present study is the high prevalence of negative mood states (19%) among 14- to 16-year-olds, particularly among girls (25%). The factor most often associated with a negative mood state was use of tranquilizers. Other factors notably associated with this negative state were eating disorders and psychological abuse. Differences were observed between boys and girls in the factors associated with a negative mood state. There was also variation among schools.
For many people, mental disorders begin very early in life1 and a greater frequency of continuity from adolescence to adulthood is increasingly being observed.23,24 Depressive disorders are common during adolescence,2 and data suggest that depressive symptomatology has increased and new diagnoses have become prominent.2 As in other studies, we observed a high prevalence of negative mood states among adolescents aged 14 to 16 years (19%), with a higher frequency in girls (25%).3,7,25,26 The items that denoted a negative mood state were similar to those reported by other studies.10,20 Negative emotional traits, with the exception of feeling threatened, were strongly associated with girls,3,27,28 coinciding with the results of Ahonen et al.8
In our study, the strong association between a negative mood state and the use of tranquilizers in both boys and girls was particularly noteworthy. Most of the studies that have addressed depressive symptomatology and the pattern of illegal substance abuse in adolescents did not include tranquilizers among their variables, although some studies, such as that by Obando et al,29 have reported this association. Our study did not determine whether this use was medically prescribed or “self-prescribed”. In recent years, a worldwide increase has been observed in self-prescription of these substances in adolescents30,31 especially in girls.32 The main source of access are friends in the United States and the family in Europe.15 This use could be related to a pattern of problem behaviors that hamper the determination of a primary cause in a cause-effect relationship.32 The increased use of tranquilizers in adolescents observed in other studies, as well as the association between the use of tranquilizers and negative mood states found in our study and in a few other previous studies29 raises the need for future research aimed at understanding and preventing this behavior.
Differences between genders were found in the factors related to negative mood states. In girls, the most significant factors associated with reporting negative mood states were “use of tranquilizers” and “having an eating disorder”, while in boys these factors were “no exercise” and “having poor self-perception of health status”. Our results do not agree with those of Ahonen et al.,8 Haarasilta et al.,4 or Saluja et al.3 However, these studies differ from ours in study design, including methodology, age of the students and adjustment variables, hampering comparison of the results.
Our study of negative mood states identified several factors associated strongly and exclusively with female sex: the use of alcohol, sexual abuse and low academic performance. We observed a relationship between negative mood states and the use of alcohol, which coincides with the findings of other studies,4,7,8,33 especially in girls, as also reported by others.3 However, unlike other studies, we found no association with other addictive substances. This finding could be due to differences in sample size,8,20 the data collection method,7 or the definition of variables,7 hampering comparison of the results. Nonetheless, this increased association in adolescent girls, which has been reported in multiple studies, points to the need to explore the news trends, roles and patterns of alcohol consumption. In concurrence with other studies, the results of our study also show that negative mood states in girls have a highly positive association with low academic performance8 and sexual abuse.27
In addition, our study shows an association between negative mood states and not exercising, especially in boys. This relationship suggests that physical activity could be a protective factor for mental health, as demonstrated in other studies.34,35 Never exercising or exercising only occasionally were associated with negative mood in a study by Haarasilta et al.4 However little research has assessed self-perception of health in adolescents and further studies are needed to explore this topic.
Independently of gender, our results showed a highly significant positive association between negative mood states and eating disorders (SCOFF), as observed in previous studies,36 while students who perceived psychological abuse were twice as likely to report having a negative mood state. Several studies suggest that psychological abuse can have adverse effects on mental health37 and is related to the presence of depressive symptoms in adults.38 Other factors associated with negative mood states in both genders were bullying and antisocial behavior. In the case of bullying, both being the victim and being the aggressor showed a strong positive association with the odds of having a negative mood state, especially in students who reported being the victim. Fekkes et al.39 reported a strong association between being a victim and depression, while in a study by Saluja et al.3 aggressors reported a greater proportion of depression. These contradictions show the need for further research on the subject.
Finally, variability was found among the various schools in the negative moods of adolescents. When adjusted by student characteristics, variability was greatly reduced in both genders; however, the variability among schools persisted and cannot be explained by any of the variables studied. Additional features of the adolescents, the schools or contextual factors that could account for the differences among schools should be studied. Future research emphasizing possible interventions that could be implemented in schools, as well as possible preventable factors, is required.
One possible weakness of our study is the use of self-administered questionnaires, which could have introduced biases in the evaluation of behaviors either because some behaviors are difficult to remember or because some adolescents do not want to talk about them. However, other means of administration could have increased the probability of information biases, especially in questions influenced by social desirability. Another possible limitation is that we used an adaptation of the self-administered Risk Factors in Barcelona Schoolcildren [Factors de Risc en Escolars de Barcelona (FRESC)] questionnaire developed by Barcelona's Public Health Agency. This is a generic health questionnaire that was not specifically designed to measure mental health. The questions about mood states existed in the original questionnaire and have been used in other studies to measure aspects related to mood states in adolescents.8 This generic questionnaire that measures various aspects related to the health of this population group was not used with the intention of screening to estimate the possible prevalence of depression, but rather to detect the symptoms most relevant to mental health in adolescents. A final consideration is that other school variables that could have accounted for the differences among schools were not available at the time of the analysis.
Despite these limitations, our study had several strengths consisting of a population-based design, a large sample size, a large number of factors possibly associated with the outcome, and random-effects modeling. Compared with experimental or interventional studies, results based on data representative of Catalonia's student population provide greater confidence in the external validity of the findings. The multilevel methodology allowed us to study not only individual variables, but also possible contextual variables that could influence the variability in the outcome, which other classical models of analysis cannot explore.
Mood disorders, especially depression, are a frequently undiagnosed and under-treated problem in adolescents. Various studies have identified some factors associated with mental health problems. However, only a few studies have evaluated these factors together.
What does this study contribute to the literature?The prevalence of negative mood states in adolescents is high, especially in girls. The most strongly associated factors are the use of tranquilizers, eating disorders and psychological abuse. There are differences between boys and girls in the factors associated with negative mood states.
M. Monteagudo, T. Rodriguez-Blanco, M.J. Pueyo, M. Mercader, E. Zabaleta-del-Olmo and B. Bolíbar contributed to the conception and design of the study represented by the article or analyzed and interpreted the data. All authors participated by drafting the article or critically revising it for important intellectual content and by giving final approval of the version to be published.
FundingHealth Department, Catalan Government, Catalonia, Spain.
Conflict of interestNone.
The authors thank all the participating schools, and the interviewers. We would also like to thank José García (Directorate-General of Planning and Assessment, Department of Health of Catalonia, Mental Health Master Plan, Barcelona, Spain) and Enriqueta Pujol (Institut d’Investigació en Atenció Primària Jordi Gol [IDIAP Jordi Gol], Barcelona, Spain) for reading and providing advice on the manuscript, as well as IDIAP Jordi Gol and Mamta Advani for their support in correcting the translation.











