



Older adults are seldom considered in studies on the health impact of economic recessions or crises. However, they constitute a population group that is highly vulnerable to decreases in investment in health and social services and social security. Our aim is to examine the relationship between the economic crisis starting in 2008 and the health status of older adults in Spain. More specifically, we analyze changes in trends of mortality in relation to the crisis, the specific impact of winter on mortality and gender differences in the crisis’ impact on mortality. Using data from the National Institute of Statistics of Spain on people over 60 years of age, the number of monthly deaths by age and sex from January 2005 to December 2012 was analyzed. Interrupted time series analyses and the “difference in differences” method were used. During the crisis, for adults 60 years and older: 1) the observed mortality seems to be decreasing at a slower rate than what would have been expected in the absence of the crisis; 2) there has been an increase in winter mortality; 3) the impact of the crisis has been greater for female than for male mortality. These results suggest sizable effects of the economic crisis on the mortality of older adults and argue for research done using more detailed analyses integrating economic indicators.
Las personas mayores son rara vez consideradas en los estudios sobre los impactos sanitarios de las recesiones o crisis económicas a pesar de constituir un grupo de población vulnerable a las disminuciones de inversión en la oferta de servicios o a las cotizaciones sociales. Nuestro objetivo es examinar la relación entre la crisis económica iniciada en 2008 y la salud de la personas mayores en España. Se analizan los cambios en las tendencias de mortalidad en relación a la crisis, su impacto específico en la mortalidad invernal, y las diferencias de su impacto entre hombres y mujeres. Utilizando datos del Instituto Nacional de Estadística, se analizan las defunciones mensuales por edad y sexo (a partir de los 60 años) desde Enero de 2005 a Diciembre de 2012. Se realiza un análisis de series temporales interrumpidas y un análisis del tipo “diferencias de diferencias”. En personas mayores de 60 años y en el periodo de la crisis en curso: 1) la mortalidad observada parece disminuir más lentamente de lo que se hubiera esperado en ausencia de la crisis; 2) un aumento en el exceso de la mortalidad invernal y 3) un impacto más importante de la crisis en la mortalidad de las mujeres que en los hombres. Estos resultados sugieren efectos importantes de la crisis económica en la mortalidad de las personas mayores, así como pistas de investigación que se podrían explorar con análisis más detallados integrando indicadores económicos.
Key ideas
During the 2008-2013 crisis, for adults 60 years and older in Spain:
- •
The observed mortality seems to be decreasing at a slower rate than what would have been expected in the absence of the crisis.
- •
There has been an increase in winter mortality.
- •
The impact of the crisis has been greater for female than for male mortality.
Older adults have been seldom considered in studies of the health impacts of economic crises. However, the austerity measures that have been imposed during the economic crisis of 2008 have limited social protections. Social services, such as home care and day care1, and services for people with dependency linked to disability, included in the Law of Protection of people in dependency situations have been reduced2. There has been a reduction in health services3 and out of pocket payments have been implemented for some services. Retirement and Old Age pensions have not been adjusted to the cost of living and consumer purchasing power is reduced1,4 In addition, older adults have often become the greatest source of economic support for the younger members of the family and the main source of care for children and disabled family members. It is also very likely that the vulnerability of older adults to austerity measures is exacerbated among women. Older women are more affected by poverty because their pensions are lower than those of men, given lower contributions to Social Security and less qualified jobs or smaller salaries for comparable jobs. In addition, personal care for family members and house work, all informal labor, are usually the responsibility of the women in the family as more than 80% of caregivers are women5
Given the sparse data available to assess physical and mental health changes in populations during an economic crisis, all-cause mortality can be used as a first approximation to detect changes and to propose research questions on vulnerable groups. Change in mortality rates of older adults should capture important austerity effects on health. However, it is necessary to take into account that in Spain, as in all high income countries, there is a strong historical trend of increasing life expectancy and a reduction of mortality at every age6. It is thus possible that austerity measures do not lead directly to a decrease in life expectancy but to a slowdown in the increase of life expectancy; in other words, the observed mortality rates during the crisis will be higher than what would have been expected if the rate of mortality reduction had remained unchanged. Our hypothesis on the slower rate of increase in life expectancy in the older population was motivated by the reduction in the life expectancy in Spain during 20126. This observation, coupled with the fact that almost 90% of all deaths in 2012 occurred in persons aged over 60 years, has led us to examine the changes in mortality before and after the crisis in older adults in Spain.
It is well known that mortality rates are higher in winter7. We formulate the hypothesis that changes in mortality will be more noticeable in the winter months. An increase in winter mortality could be due to the increase of prices of home heating during the crisis. This phenomena, described in the United Kingdom as “fuel poverty”, is more frequent in the homes of older adults8,9. It is thus necessary to take into account the fact that in Spain the price of electricity has increased 63% from 2003 to 2011 and 8% from January 2012 to August 201310. It is likely that what has been observed in the UK is also happening in Spain.
The aims of this paper are: 1) to document the change of trends in mortality in adults aged 60 years and over in the years before and after the crisis; 2) to observe these trends during the winter; and 3) to analyze if these changes are different by age group and sex. Our hypotheses are: i) during the crisis of 2008-2013 a slowdown in the decreasing mortality trend has been observed in adults over 60 years of age; and ii) changes in mortality trends are larger in women than in men of comparable age.
MethodsDataWe used monthly mortality rates by age (starting from 60 years old) and sex from January 2005 to December 2012 using data available from the Spanish National Statistics Institute11. Mortality rates were obtained for the whole of Spain. Age groups were stratified into three groups: 60-75, 76-90, and 91 and older. The winter period was defined as the months from December to March. We considered that the financial crisis began in 2008 and we compared the before-crisis period (defined as 2005 to 2007) to the economic crisis period (defined as 2008 to 2012).
Statistical AnalysisPart 1: Change in mortality rate trends
To analyse trends in mortality rates, we conducted three different analyses. 1) First we compared the monthly mortality rates in the pre-crisis and crisis periods using paired t-tests12. 2) Then, we conducted two separate linear regressions to estimate the association between the time trend and mortality rates, one for pre-crisis period, and another for the crisis period. We compared the two coefficients to test the hypothesis of a decline in the historically decreasing rate of mortality. 3) Finally, we conducted interrupted time series analysis, taking into account secular time trends and annual variations. The model adjustment method followed the procedure suggested by Donnelly13. Both analyses were conducted for all ages and then stratified for the different age groups.
Part 2: Changes in winter mortalityWe compared the mortality rates between the winter months (December to March) and other months on the one hand for the pre-crisis period and on the other hand for the post-crisis period using a paired t test. We then applied a “difference in differences” method (DID), which is often used in econometrics to assess changes after and before a specific event. Here we compared the difference between winter months and other months before the crisis (2005-2007) and after (2009-2012). We used monthly mortality rates by age groups and sex to obtain DID estimates with the following formula:
DID i, j = [(MR winter – MR other seasons] crisis– [MR winter’ – MR other seasons’] before crisis
Where MR is the mortality rate for age group i and sex j
Part 3: Crisis-related mortality differences between men and womenWe used the DID method separately for men and women for the winter period to assess a potential heterogeneity between sexes. We then conducted the same analyses independently for the three age groups (i.e. for six strata of age and sex). Finally, we conducted an interrupted time series analysis with the created variable diffsex (MR men - MR women) as the outcome, in order to assess the crisis’ impact on mortality rate differences between sexes.
ResultsDuring the study period 2,704,700 deaths were observed, with a monthly average of 32,199 deaths (60 years and over), a maximum of 35,172 deaths for the month of February and a minimum of 27,818 deaths in September. The monthly average death rate was 35 per 100,000 for the 60 to 75 age group, 169 per 100,000 for the 76-90 age group and 1237 per 100,000 for those aged 91 and over.
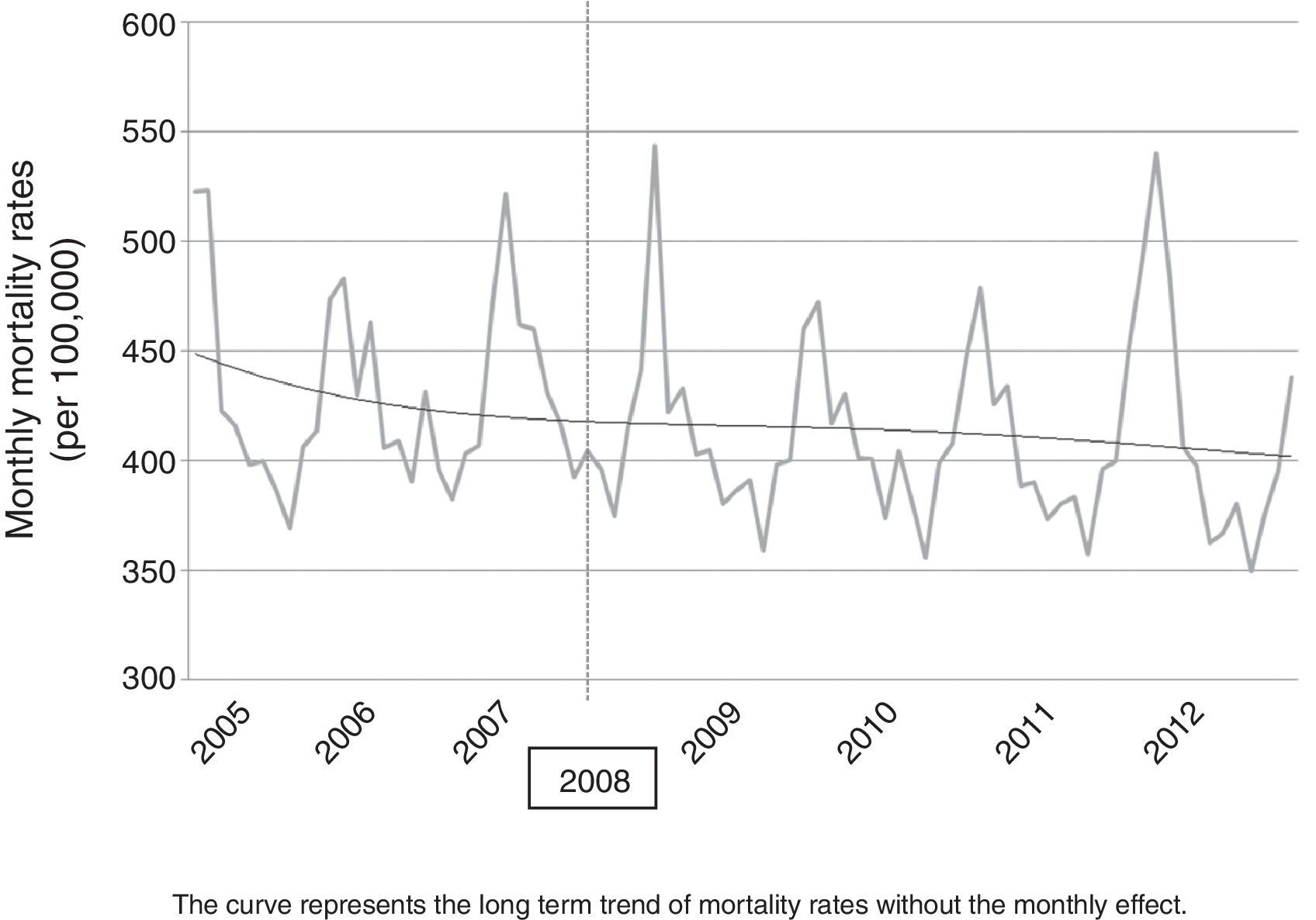
Part 1. Changing trends in mortality rateFigure 1 shows trends in mortality rates in the pre-crisis period and during the crisis. There is a general decline in the mortality rate over the entire study period. Looking at the trend line representing no monthly effects, a decrease in the slope from 2008 (beginning of the crisis) is apparent. To verify that mortality rates differ by month, we conducted t-tests for paired samples. The results for the entire population and for each age stratum are significant (p<0.01 in both cases). This means that paired mortality rates per month are different before and after the crisis.

We performed two linear regressions, one for the pre-crisis period and the other for the crisis period. The coefficient for the pre-crisis period corresponds to a decrease of 0.38 deaths per 100,000 per month while in the crisis period this coefficient was -0.005, i.e. a decrease of 0.005 per 100,000 per month, which is negligible. This demonstrates a slower (though practically negligible) decrease in the annual mortality rate during the crisis.
To complete these analyses, interrupted time series analysis on the long-term series was carried out.
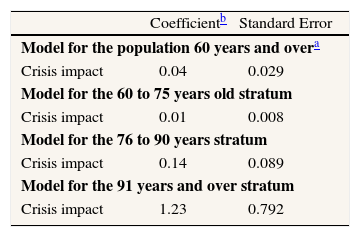
Table 1 shows the results of the impact of the crisis on trends in mortality rates. For the entire study population (all strata), the crisis has the effect of increasing the death rate by 0.04 per 100,000 per month, compared to what would be expected if there had been no crisis. These coefficients increase with age strata, 0.01, 0.14 and 1.23, respectively, for the strata (60-75), (76-90) and (91 and over).
Change in the trends of monthly mortality rates before and during the crisis: Interrupted time series analyses results.
Here we have restricted the analysis to the winter period. Paired mortality rates for the winter period are significantly different from the pre-crisis period and the crisis period (p<0.01).
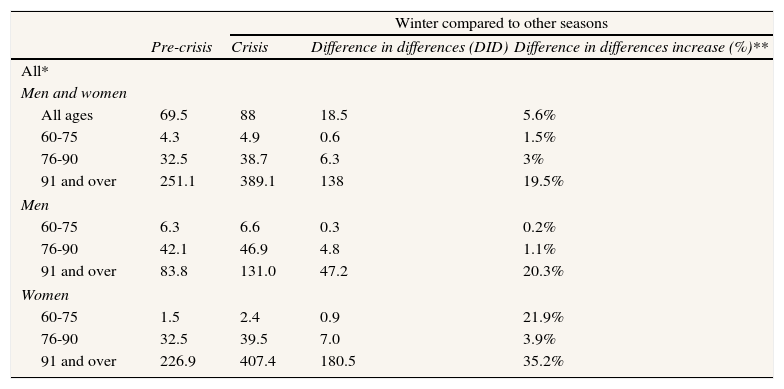
We performed analysis of difference-in-differences (DID), comparing the winter period with the rest of the year in both pre-crisis and crisis periods. The results expressed in absolute DID increases and in % for the entire population and for each age group; they are shown in Table 2. It can be observed that mortality rates are higher in winter than in other months of the year, and this seasonal difference is systematically more pronounced during the crisis than before the crisis. For example, for the stratum of 76 to 90 year-olds, the DID is 6.3 and the DID percentage increase is 3%. Overall, winter mortality has increased for people over 60 years old since the beginning of the crisis.
Estimation of the difference in differences increase of monthly mortality rates between winter and other seasons, before and during the crisis.
| Winter compared to other seasons | ||||
| Pre-crisis | Crisis | Difference in differences (DID) | Difference in differences increase (%)** | |
| All* | ||||
| Men and women | ||||
| All ages | 69.5 | 88 | 18.5 | 5.6% |
| 60-75 | 4.3 | 4.9 | 0.6 | 1.5% |
| 76-90 | 32.5 | 38.7 | 6.3 | 3% |
| 91 and over | 251.1 | 389.1 | 138 | 19.5% |
| Men | ||||
| 60-75 | 6.3 | 6.6 | 0.3 | 0.2% |
| 76-90 | 42.1 | 46.9 | 4.8 | 1.1% |
| 91 and over | 83.8 | 131.0 | 47.2 | 20.3% |
| Women | ||||
| 60-75 | 1.5 | 2.4 | 0.9 | 21.9% |
| 76-90 | 32.5 | 39.5 | 7.0 | 3.9% |
| 91 and over | 226.9 | 407.4 | 180.5 | 35.2% |
* Mortality rates per 100.000 people.
** The DID percentages increases were obtained following the method used by Cutler et al., 2000. by comparing the ratios of differences between periods (pre-crisis vs. crisis). For example. for both sexes and all ages. the difference in differences between periods was (88-69.5) = 18.5 and the DID percentage increase was (18.5/69.5)-(18.5/88) = 5.6%.
Part 3 Mortality differences between men and women in relation to the crisis
We then studied the impact of the economic crisis on the difference in mortality between men and women. The average number of deaths in women was 1744 deaths per month before the crisis and 1835 during the crisis. The average number of deaths per month was 1637 in men before the crisis and 1700 during the crisis. The overall monthly death rate during the study period 2005-2012 was 452 deaths per 100,000 in women and 554 deaths per 100,000 in men.
We also carried out a DID analysis comparing changes in mortality rates before and during the crisis among men and women (Table 2). We see that the results are different between the two sexes, which shows that the crisis has a differential impact on older men and women. With the exception of the age group aged over 90, winter mortality is higher in women than in men; this gender difference is accentuated in the period of crisis.
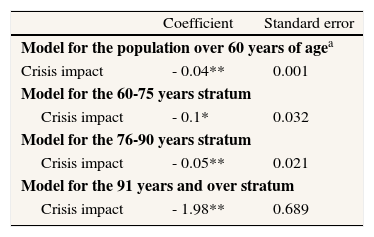
To analyze this difference between the sexes, we created a variable, “diffsex”, which corresponds to the difference of the monthly mortality between men and women. We then used interrupted time series analysis to analyze the impact of the crisis on mortality trends between men and women. The results of the crisis’ impact on the trend of the differences in mortality rates in men and women are shown in Table 3. The crisis has significantly decreased the difference in mortality rates between men and women at 0.04 deaths per month. In other words, these results show that during the crisis, mortality rates in women decrease more slowly than in men with the result that the difference in mortality between the sexes has decreased, to the point of losing statistical significance.
Crisis impact on the trend of the differences in mortality rates in men and women.
| Coefficient | Standard error | |
| Model for the population over 60 years of agea | ||
| Crisis impact | - 0.04** | 0.001 |
| Model for the 60-75 years stratum | ||
| Crisis impact | - 0.1* | 0.032 |
| Model for the 76-90 years stratum | ||
| Crisis impact | - 0.05** | 0.021 |
| Model for the 91 years and over stratum | ||
| Crisis impact | - 1.98** | 0.689 |
a Models are adjusted for the effect of the crisis, long term trends, yearly trends and interaction between the crisis and the long term trends.
*: P<0.05; **: p<0.01.
In this study of mortality of older adults in Spain, we have shown the possible impact of the economic crisis since 2008. Our results suggest that a deceleration in the decrease of mortality rates occurred with the crisis; secondly, they show that the impact of the crisis on mortality can be greater in the winter months than in the remaining months of the year. Also, the mortality of older women has suffered greater change than the mortality of men of comparable age.
Several studies have examined the link between the economic crisis with their associated austerity measures and their impact on the health of the population. In this study we have obtained results similar to previous studies in contexts as different as South Korea14,15 and Mexico16, although we have restricted our attention to the population of older adults and we have only analyzed all-cause mortality. We have used the method of differences in differences, a method known in this field, and interrupted time series analyses because they enable control of annual or monthly mortality trends.
This crisis that struck Europe in 2008 is certainly a crisis of an economic nature but it is also a crisis of the social system, that is to say, a crisis of values. One could accept, although this is a subject for debate in the economic sciences, whether economic crises are unavoidable, but the choice of austerity measures, in the way they have been chosen in Spain, is indubitably an avoidable one. Studies on the health impact of economic crises have shown the diversity of their effects. These effects depend primarily on the contextual features of the country, both in relation to existing social policies and to the cultural and social values in which these policies are grounded. However, it seems that the health impacts of economic crises depend strongly on the political response of the governments that face these crises17,18. Some authors state that to a great extent, austerity measures could well explain the effects of the crisis on the health of the population, and to a minor extent the actual crisis. In fact, Karanikolos et al.19 have shown that Portugal, Greece and Spain, countries adopting a strict fiscal policy, have suffered the strongest effects on the population's mortality, morbidity and well-being19–21. In contrast, Iceland, who rejected austerity measures based on a popular vote, has not experienced an impact on the public's health and has even observed improvements in some population health indicators21–23.
Alternative policies, such as disinvestment, have received little consideration by the proponents of austerity, even if they would have had an impact on population's health and wellbeing and these impacts could have been quantified over a long-term period. This idea has already been developed by Dávila Quintana y Gonzalez López-Valcárcel17 who proposed that it was more the austerity measures than the crisis itself that had effects on the health of the population. Thus, in the study of the impacts of the European economic crisis and the austerity measures applied to palliate its effects, Spain constitutes a compelling case study.
This study deals with all-cause mortality in the whole territory of the State of Spain in the context of a diffuse phenomenon such as the economic crisis. This broad aim leads us to some questions on its methodological limits and the validity of the results. The general changes in mortality that we have unveiled do not allow us to conclude on a change in mortality of the elderly population during the economic crisis but they have identified marked changes in the winter period and the larger mortality change in women. Here, we have examined all-cause mortality but future studies should investigate specific causes as has been previously done14,24. Even if we have not been able to use a long series of mortality or daily mortality rates, we have used at least two different methods of analysis for each of the three sections. This helps to avoid bias25 and strengthens the evidence for the hypothesis we propose. We have considered that the crisis started in 2008 but it is difficult to establish the precise moment at which the crisis’ effects started to manifest. Future research could examine the changes in the Gross National Product in relation with the mortality and the life expectancy of older adults before, during and after the crisis in Spain. Besides mortality, the impact of the crisis on morbidity (for example, hospitalizations, infectious disease incidence, cancer survival), social cohesion and quality of life of older adults could be examined. Lastly, the main limitation of our study is that we cannot attribute the observed changes in mortality to the crisis or to the austerity measures because we have not integrated economic indicators of the crisis or of the austerity measures in our analyses.
With the caution that the above limitations require, the observed changes in mortality lead us to suggest that there have been changes in the health of older adults due to a worsening in their life conditions and/or in the access and quality of the services that they are offered. The increase in the risk of dying in relation to what was expected in absence of the crisis is an indicator of an increase in physical and mental health conditions, and in consequence increases in disability. It behoves us to remember that the improvements in health and functional capacity observed in the elderly population of Spain during the last years of the 20th century are not permanent gains and that these improvements are not irreversible. A worsening of living conditions and a reduction in health and social services would be sufficient for the worsening of the health of older adults. Our results support the hypothesis that the effects of the management of the crisis are already detectable in mortality rates, one of the few available indicators to assess the crisis’ effects on the health of older adults in the territory of Spain.
Based on our results, we propose four mechanisms to explain how the health of older adults could be particularly vulnerable to the crisis management methods used in Spain:
- 1.
The reduction of health and social services3
- 2.
The decrease in consumer purchasing power of old age pensions and the increase in poverty, even more critical when old age is accompanied by disability26,27
- 3.
Psychosocial and economic stress since older adults have become the main source of support for the family, due to the return of adult children to the parental home, which is in turn due to a lack of work opportunities for young adults, under extremely high unemployment rates which hinder their career development4.
- 4.
The informal house work and care that older adults need to carry out for younger members of the family, such as looking after grandchildren and caring for disabled and sick family members.
Improving our understanding of the effects of the crisis on the health of older adults is the first step toward prevention. More specific research will be needed to advance knowledge of the mechanisms by which winter effects and gender inequalities operate. Among the actions to be encouraged, we insist that inter-sectorial interventions to promote active aging are particularly relevant in times of crisis28. Disability prevention, economic security and social participation are the pillars of active aging, a process that will cost less to society while providing the quality of life worthy of the elderly, who have contributed to our society for their entire life.
AuthorshipT Benmarhnia contributed to defining the research question, conducted the data analysis and wrote the first version of the paper. MV Zunzunegui contributed to formulating the hypothesis, to the interpretation of results, to the discussion and to several previous versions. Alicia Llácer y François Béland contributed to the original conceptualization of the research question, to the interpretation of results and to the writing of several versions.
Funding sourcesNone
Conflict of interestThe authors have no conflicts of interest to declare.











