




To evaluate the effectiveness of ImpactReel, a universal school-based program that integrates social media literacy, self-compassion, and acceptance strategies to improve body image and reduce risk factors for eating disorders in adolescents.
MethodA two-arm cluster randomized controlled trial (intervention vs. waitlist) will be conducted with first-year secondary school students in Spain. The intervention consists of one weekly 55-minute session for seven weeks delivered by trained psychologists, combining social media literacy with principles of compassion-focused therapy and acceptance and commitment therapy. Assessments will be conducted at four time points: pre-intervention, post-intervention, and follow-ups at 6 and 12 months. The primary outcome will be body esteem, and secondary outcomes will include self-compassion, internalization of appearance ideals, social media literacy and use, eating disorder risk, depressive symptoms, and life satisfaction.
Evaluar la eficacia de ImpactReel, un programa escolar universal que integra alfabetización en redes sociales, autocompasión y estrategias de aceptación, para mejorar la imagen corporal y reducir factores de riesgo de trastornos de la conducta alimentaria en adolescentes.
MétodoSe llevará a cabo un ensayo controlado aleatorizado por conglomerados con dos grupos (intervención frente a lista de espera) en estudiantes de primer curso de secundaria en España. La intervención consta de una sesión semanal de 55 minutos durante 7 semanas impartida por psicólogos/as, combinando alfabetización en redes sociales con principios de terapia centrada en la compasión y terapia de aceptación y compromiso. Las evaluaciones se realizarán en cuatro momentos: preintervención, posintervención y seguimientos a 6 y 12 meses. La variable principal será la estima corporal, y como variables secundarias se evaluarán la autocompasión, la internalización de ideales de apariencia, la alfabetización y el uso de redes sociales, el riesgo de trastornos alimentarios, los síntomas depresivos y la satisfacción vital.
Body dissatisfaction, defined as a negative assessment of physical appearance, is a well-established risk factor for eating disorders.1 During adolescence, body dissatisfaction is highly prevalent, affecting both girls and boys, although clinically significant levels are more frequent among girls.2 Evidence from systematic reviews indicates that negative body image is associated with a wide range of adverse outcomes, including dieting, restrictive eating behaviours, excessive exercise, and poorer psychological well-being.3,4
Sociocultural models have long highlighted the role of cultural pressures and media exposure in shaping body image concerns. The tripartite model of body image and objectification theory emphasises the influence of media, peers and family in promoting unrealistic appearance ideals and the internalisation of beauty standards.5,6 In recent years, social media has become a central factor within these frameworks, as adolescents increasingly engage with visually oriented platforms that facilitate constant exposure to idealised images and appearance-focused interactions.7
Systematic reviews and meta-analyses consistently show that greater social media use is associated with higher levels of body dissatisfaction among young people.8,9 These associations appear to be partly explained by mechanisms such as upward social comparison and the internalisation of appearance ideals frequently promoted in online environments.10 Adolescence represents a particularly vulnerable developmental period in this context, as it is characterised by heightened sensitivity to peer evaluation and intensive engagement with digital media.
Given the growing concern about the impact of social media on adolescent well-being, several prevention programmes have been developed to address body image concerns in school settings. Evidence from meta-analytic reviews indicates that such interventions can produce small to moderate improvements in body image outcomes and media literacy, although effects are not always consistent across studies.11,12 Moreover, relatively few programmes specifically address social media environments, and many interventions have been criticised for limited long-term effects and insufficient attention to gender differences in body image concerns.
Emerging psychological approaches, such as acceptance and commitment therapy and compassion-focused therapy, have shown promise in addressing body dissatisfaction by targeting key mechanisms including self-criticism, shame and rigid appearance-based self-evaluation. In particular, self-compassion has been identified as a protective factor that may buffer the impact of social comparison and promote more adaptive body image and psychological well-being.13,14
Considering that body image concerns manifest differently across genders, often involving thinness ideals among girls and muscularity concerns among boys, it is important that prevention programmes adopt gender-sensitive approaches capable of addressing diverse appearance pressures during adolescence.
The present study introduces ImpactReel: The Impact of Social Media on Body Image, a universal school-based prevention programme designed for early adolescents that integrates social media literacy with mindfulness, acceptance and self-compassion strategies. The objective of this study is to describe the protocol of a cluster randomized controlled trial designed to evaluate the efficacy of the ImpactReel programme in improving body image and reducing risk factors associated with eating disorders among adolescents.
MethodEthical considerations and trial registrationThe project and data collection were authorized by the Department of Education of the Valencian Regional Government (240115174018) and approved by the Office of Responsible Research of Miguel Hernández University (SPU.MJQS.SFG.24). It has also been registered with the Clinical Trials Registry (NCT07103213). The study will be conducted in accordance with the Declaration of Helsinki and relevant national regulations.
Before the implementation of the study, authorisation must be obtained from the participating centres by the management team. Prior to participation, written informed consent will be obtained from both students and their legal guardians. Participation will be voluntary, and students may withdraw at any time without consequences. Data will be collected using pseudonymised codes to ensure participant confidentiality. All data will be securely stored and handled in compliance with data protection regulations.
Facilitators will be trained to identify signs of distress and to respond following established safeguarding protocols. No incentives will compromise voluntary participation, and confidentiality will be emphasized throughout the study.
Study designThis multicentre cluster-randomized controlled trial will evaluate the effectiveness of the school-based programme ImpactReel. Classes will be assigned to either the intervention or a waitlist control group. The intervention group will receive one weekly session for seven weeks, and outcomes will be assessed before, after, and at six- and twelve-month follow-ups.
MeasuresDemographic informationSociodemographic data will include participants’ high school and class, as well as their gender (options: female, male, other) and age. In addition, participants will self-report their weight (kg) and height (cm).
Social media use and lifestyle variablesParticipants will report their estimated daily mobile phone use and the social media platforms they use most frequently, as well as the number of weekly hours spent in extracurricular sports activities and whether they have previously followed a diet, including the main reason for doing so.
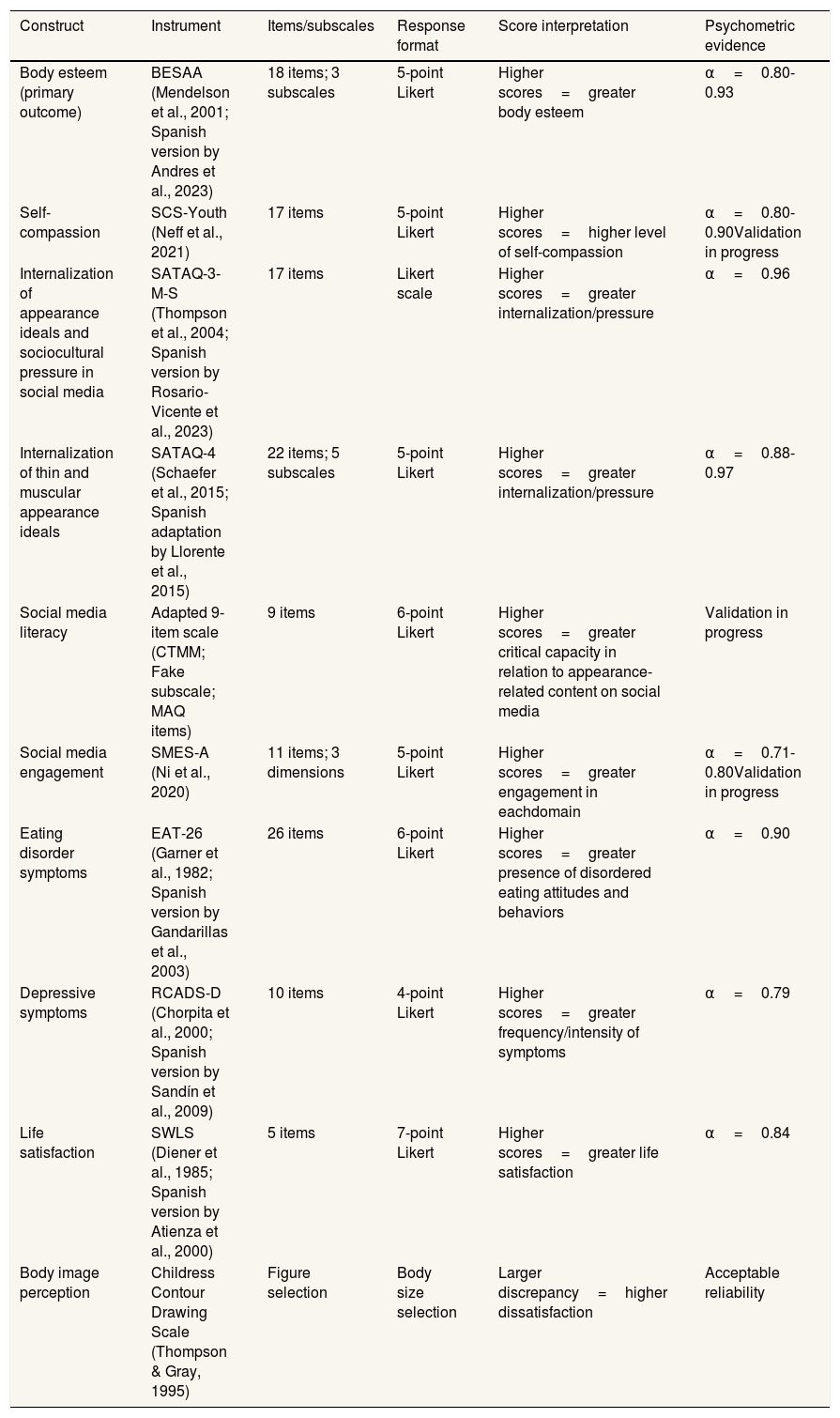
Primary and secondary outcome measuresAll assessment instruments and their psychometric properties are detailed in table 1. The primary outcome is the change in body esteem, defined as the total score of the Body-Esteem Scale for Adolescents and Adults (BESAA), specifically at the post-intervention time point (1–2 weeks after the program).
Standardized instruments used in the study.
| Construct | Instrument | Items/subscales | Response format | Score interpretation | Psychometric evidence |
|---|---|---|---|---|---|
| Body esteem (primary outcome) | BESAA (Mendelson et al., 2001; Spanish version by Andres et al., 2023) | 18 items; 3 subscales | 5-point Likert | Higher scores=greater body esteem | α=0.80-0.93 |
| Self-compassion | SCS-Youth (Neff et al., 2021) | 17 items | 5-point Likert | Higher scores=higher level of self-compassion | α=0.80-0.90Validation in progress |
| Internalization of appearance ideals and sociocultural pressure in social media | SATAQ-3-M-S (Thompson et al., 2004; Spanish version by Rosario-Vicente et al., 2023) | 17 items | Likert scale | Higher scores=greater internalization/pressure | α=0.96 |
| Internalization of thin and muscular appearance ideals | SATAQ-4 (Schaefer et al., 2015; Spanish adaptation by Llorente et al., 2015) | 22 items; 5 subscales | 5-point Likert | Higher scores=greater internalization/pressure | α=0.88-0.97 |
| Social media literacy | Adapted 9-item scale (CTMM; Fake subscale; MAQ items) | 9 items | 6-point Likert | Higher scores=greater critical capacity in relation to appearance-related content on social media | Validation in progress |
| Social media engagement | SMES-A (Ni et al., 2020) | 11 items; 3 dimensions | 5-point Likert | Higher scores=greater engagement in eachdomain | α=0.71-0.80Validation in progress |
| Eating disorder symptoms | EAT-26 (Garner et al., 1982; Spanish version by Gandarillas et al., 2003) | 26 items | 6-point Likert | Higher scores=greater presence of disordered eating attitudes and behaviors | α=0.90 |
| Depressive symptoms | RCADS-D (Chorpita et al., 2000; Spanish version by Sandín et al., 2009) | 10 items | 4-point Likert | Higher scores=greater frequency/intensity of symptoms | α=0.79 |
| Life satisfaction | SWLS (Diener et al., 1985; Spanish version by Atienza et al., 2000) | 5 items | 7-point Likert | Higher scores=greater life satisfaction | α=0.84 |
| Body image perception | Childress Contour Drawing Scale (Thompson & Gray, 1995) | Figure selection | Body size selection | Larger discrepancy=higher dissatisfaction | Acceptable reliability |
Students’ participation, including homework completion and self-reported satisfaction, will be recorded to provide context and explore associations with study outcomes. Programme satisfaction and aspects related to programme delivery will also be explored through focus groups with participants where feasible.
RecruitmentThe study will include first-year secondary school students from randomly selected schools in Elche, Spain, representing different types of institutions and socioeconomic contexts. After obtaining consent from students and their legal guardians, two classes per school will be selected by school administration, based on availability and logistical considerations, and subsequently randomly assigned to either the experimental group or a waitlist control group.
Participants and eligibility criteriaInclusion criteria are being a first-year secondary school student and providing informed consent from both the participant and their legal guardian. Students showing severe eating disorder symptoms, defined as scoring above 20 on the EAT-26 questionnaire,15 will be excluded and referred to appropriate psychological services, in line with NICE guidelines, which recommend psychological treatment as the first-line approach rather than preventive interventions.16
Given the pseudonymised nature of the data, results will be reported to participating schools at the class level (i.e., number of students at risk per class), and school guidance or counselling staff will be responsible for any follow-up actions or referrals.
Although these participants will not be included in the primary outcome analyses, their data may be retained for descriptive and exploratory purposes (e.g., to characterise the sample or examine associations between study variables). Participation in study assessments and sessions remained voluntary for all students.
Data collection proceduresThe survey will be conducted in classrooms using school computers and secure software. Participants will be assigned pseudonymised codes generated through a dedicated platform developed by Miguel Hernández University. Data will be collected over one year during school hours under supervision, and questionnaires will be completed within one class period.
Statistical power and data analysesSample size calculations will be conducted considering the cluster-randomized design of the study. To detect a moderate effect size (Cohen's d=0.50) with 80% power and a significance level of α=0.05, 128 participants (64 per group) will be required under individual randomization.17
As randomization will be performed at the class level, a design effect will be applied to adjust for within-cluster correlation. Assuming an average cluster size of 25 students and an intraclass correlation coefficient of 0.02, the resulting design effect is 1.48, increasing the required sample size to 190 participants. After adjusting for an anticipated attrition rate of 30%, the required sample size will be 271 participants.
Outcomes will be assessed at four time points: pre-intervention (1–2 weeks prior), post-intervention (1–2 weeks after, depending on school availability), and six- and twelve-month follow-ups.
Given the hierarchical and longitudinal structure of the data, analyses will be conducted using linear mixed-effects models to account for the nesting of participants within classes/schools and repeated measurements within individuals. The primary comparison will be the interaction effect between group (intervention vs. control) and time (baseline vs. post-intervention). Models will include the baseline score of the primary outcome as a covariate to maximize statistical power. Random intercepts will be included for both participants and clusters (classes) to account for correlation within these levels.
Effect sizes will be estimated from model outputs (e.g., Cohen's d or Hedges’ g) to provide standardized measures of clinical significance. Gender-based analyses will explore potential differential effects, and adherence-related models will examine the dose-response relationship. Missing data will be handled using restricted maximum likelihood estimation within the linear mixed-effects models framework. This approach provides unbiased estimates under the missing at random assumption by utilizing all available data points without the need for listwise deletion or simple imputation. Sensitivity analyses will be performed to assess the robustness of the results against these assumptions. All analyses will be conducted using IBM SPSS Statistics (version 31.0).
Randomization and blindingRandomization will be conducted at the class level within each participating school. In each school, two classes from the same grade will be included and allocated to either the intervention group or the waitlist control group. To minimize potential contamination, randomization will be conducted at the class level within schools.
The random allocation sequence will be generated using a computer-based randomization procedure by a researcher not involved in participant recruitment or intervention delivery. Allocation will be performed after class selection. Allocation concealment will be ensured as the randomization sequence will not be accessible to researchers involved in recruitment or intervention delivery until assignments are finalized.
To further reduce the risk of contamination between groups, participants in the intervention classes will be instructed not to share intervention content or materials with students in the control classes. Due to the nature of the intervention, blinding of participants and teachers will not be feasible. However, outcome assessors and data analysts will remain blinded to group allocation to minimize bias.
InterventionTheoretical basis, structure and contentThe ImpactReel programme is a school-based intervention designed to prevent body dissatisfaction in adolescents through an integrative framework combining sociocultural theory, acceptance-based approaches, and constructivist learning principles.
From a sociocultural perspective, the programme is grounded in the tripartite model of body image,6 and the sociocultural framework of development,7 which highlight the role of media, peers, and family in transmitting appearance ideals. Internalization of these ideals and social comparison processes are addressed through media literacy, psychoeducation, and critical reflection activities. Adolescents analyse manipulated images, examine marketing strategies on social media, reflect on comparison processes, and develop critical thinking skills to reduce the impact of unrealistic beauty standards.
The second theoretical pillar draws on compassion-focused therapy,18 and acceptance and commitment therapy.19 These models promote psychological flexibility, acceptance of body-related thoughts, identification of personal values, and self-compassion. The programme adopts a strictly weight-neutral perspective, emphasizing embodiment and body functionality rather than appearance evaluation. Experiential and reflective exercises help adolescents shift from avoidance- based strategies to more adaptive, values-based responses to body-related distress.
Constructivist learning principles underpin the intervention, encouraging active participation, collaborative reflection, and learning-by-doing activities that connect psychological concepts to adolescents’ lived experiences.20
ImpactReel consists of seven 55-minute sessions integrated into the secondary school curriculum and delivered by trained psychologists. Sessions include group discussions, reflective writing, role-play, guided exercises, and homework assignments to consolidate learning. The programme is gender-inclusive and incorporates examples relevant to adolescents’ current digital environments. The content and activities of each session are described in table S1 in Supplementary material online.
Engagement is reinforced through structured homework monitoring, a point-based system, and feedback, including team-based incentives. Intervention acceptability is assessed post-intervention through quantitative and qualitative student feedback.
Facilitators (pairs of psychologists) received structured training on the programme's theoretical framework, methodology, and classroom management, and delivered the sessions with shared roles to support engagement. Ongoing supervision and weekly preparation meetings were used to ensure consistent implementation and intervention fidelity across sessions.
DiscussionThe ImpactReel protocol describes a school-based cluster randomized controlled trial designed to evaluate a preventive intervention aimed at promoting positive body image among adolescents through the integration of social media literacy with mindfulness-, self-compassion-, and acceptance-based strategies. High levels of body dissatisfaction among adolescents, together with the increasing prevalence of eating disorder symptoms, highlight the urgent need for scalable and developmentally appropriate prevention initiatives.21
Previous research indicates that school-based prevention programs grounded in media literacy and cognitive-dissonance approaches are among the most effective in reducing risk factors such as thin-ideal internalization and body dissatisfaction.22 Building on this evidence, ImpactReel specifically addresses the contemporary influence of social media, a dominant context for appearance-related comparison and sociocultural pressure during adolescence. Exposure to idealized and edited images and frequent appearance-based comparison on social media are associated with poorer body image and increased risk for disordered eating attitudes.23 To address these processes, the program combines critical social media literacy with internal psychological resources, including self-compassion and acceptance-based strategies, which have shown promise in reducing self-criticism and appearance-related distress.14
A key contribution of ImpactReel to the prevention literature lies in its multicomponent approach. By targeting both sociocultural influences (e.g., unrealistic media portrayals and upward comparison) and intrapersonal protective processes (e.g., self-compassion and body acceptance), the intervention aims to simultaneously reduce risk factors and strengthen resilience. The program consists of seven manualized, facilitator-delivered group sessions implemented in the school setting, a context shown to be feasible and acceptable for preventive mental health interventions.24 The experimental design, including a control group and follow-up assessments at post-intervention, 6 months, and 12 months, will allow the evaluation of both immediate and sustained outcomes.
Based on existing evidence, it is hypothesized that adolescents participating in the intervention will show reductions in eating disorder-related risk attitudes (EAT-26 <20) and improvements in body esteem, self-compassion, and social media literacy compared with the control group. This multicomponent structure aligns with recommendations from recent prevention research emphasizing interventions that address multiple psychosocial mechanisms associated with eating disorder risk.25
Several limitations should be considered. The study relies on self-report measures, which may introduce biases such as social desirability and response fatigue. In addition, some of the instruments included have not yet been fully validated in Spanish adolescent populations, including the social media literacy measure, the SCS-Youth, and the SMES-A. However, these instruments were selected because they assess constructs directly targeted by the intervention and have shown adequate performance in previous international research. Importantly, the present study is part of a broader research project in which the validation of these instruments in Spanish adolescent populations will be undertaken. Within this framework, their psychometric properties will be examined, including internal consistency and the evaluation of their factor structure through exploratory and/or confirmatory factor analyses, as appropriate.
Finally, cultural factors related to body image norms and media exposure may limit the generalizability of the findings. Despite these limitations, implementing a brief, manualized intervention within the school context may represent a feasible and scalable strategy to promote healthier body image and reduce eating disorder risk among adolescents.
Editor in chargeSalvador Peiró.
Authorship contributionsS. Fernández García: conceptualization, funding acquisition, investigation, methodology, project administration, writing original draft, review and editing. J. Manchón López: conceptualization, investigation, methodology, project administration, supervision, writing, review and editing. M.J. Quiles Sebastián: conceptualization, investigation, methodology, project administration, resources and supervision.
FundingThis work was supported by a collaboration grant by the Government of Spain, Ministry of Universities (application No: FPU22/03291).
Conflicts of interestsNone.
The authors gratefully acknowledge the support of the Government of Spain, Ministry of Universities, through the collaboration grant (Application No. FPU22/03291) that made this work possible.












