




The aim of this paper is to study the opportunity costs (OC) that are involved in being a caregiver and to compare them with the direct costs assumed by the State and the families. We evaluate direct cost (those that imply a payment-out-of-pocket) and indirect cost (those that imply a dedication in time). We hypothesized that costs increase with the severity of the dementia, with the educational level and active occupational situation of caregiver. They are greater if the caregiver is male, but if the patient and caregiver cohabit they are reduced.
Method778 surveys were analyzed. Data was collected using a questionnaire specifically designed for the purpose, with the collaboration of Alzheimer's Diseases Associations in Andalusia (Spain). For the indirect cost, we used the reveal preferences method. For the comparison between groups an ANOVA and a MANOVA was done.
ResultsThe hypotheses were confirmed. The OC exponentially increases with severity. More than 55% of costs are assumed by families. Occupied people have higher educational level and incomes and contract more external support. Costs are significantly higher for male caregivers. Cohabiting reduces all kinds of costs.
ConclusionsThe relationship between educational level and employment situation lead to think that if these variables are greater more people will seek professional support. Cultural reasons still maintain women as main caregivers for all educational levels. The existence of these informal caregivers as the main care providers is a saving for the State, and a brake for the development of professional supply.
Estudiar los costes de oportunidad de ser cuidador, y comparar los costes directos asumidos por el Estado y las familias. Evaluamos los costes directos (los que suponen desembolso) e indirectos (los que suponen dedicación en tiempo). Planteamos la hipótesis acerca de que los costes se incrementan con la gravedad de la demencia, con el nivel educativo y con la situación laboralmente activa del cuidador. Dichos costes son superiores si el cuidador es varón, y se reducen con la convivencia.
MétodoSe analizaron 778 cuestionarios. Los datos se recolectaron mediante un cuestionario específicamente diseñado para este fin, contando con la colaboración de las asociaciones de Alzheimer de Andalucía (España). Para el estudio de los costes indirectos se usó el método de preferencias reveladas. Para la comparación de grupos se realizó ANOVA y MANOVA.
ResultadosLas hipótesis se confirmaron. Los costes de oportunidad se incrementan exponencialmente con la gravedad. Más del 55% de los costes son asumidos por las familias. Los ocupados tienen un mayor grado de formación e ingresos y contratan más apoyo externo. Los costes son significativamente superiores para cuidadores varones. La convivencia reduce todos los tipos de costes.
ConclusiónLa relación entre el nivel educativo y el empleo lleva a pensar que, si estas variables crecen, un mayor número de personas buscará apoyo profesional. Las razones culturales mantienen a las mujeres como cuidadoras principales, independientemente del nivel formativo. La existencia de estos cuidadores informales como principales proveedores de cuidados suponen un ahorro para el Estado y un freno para el desarrollo de la oferta profesional.
Dementia is an acquired organic syndrome that leads to a continuous deficit of the cognitive functions. In this evolution, there are other complications that affect the emotional, behavioural and psychiatric spheres. Motor limitations are also affected during the severe stages, although depending on the type of dementia these symptoms can appear earlier.1,2
There are some risk factors linked to habits or lifestyle (alcohol, sedentarism, diabetes).3,4 Some of them are linked to socio-economic factors, and therefore potentially modifiable. Modifying these risk factors can alter the risk of dementia and the associated costs.5 There are also other factors such as gender, age,6,7 or genetic factors that are impossible to change.
The most prevalent type of dementia is Alzheimer's Disease (AD).7 People with dementia need to be cared for. In this paper, we focus on informal caregivers. We will consider informal caregivers non-professionals who provide care. In our sample, we require they be the main caregiver for at least six months a year.
Prevalence doubles on average every 5.5-6.7 years among those over 60 years old.8 The total amount of people with dementia in the world could be 115.4 million by 2050.8 In Spain, there are around 10 million people over 60. 35.9% of them could already be in a preclinical stage of Alzheimer's disease.9 The estimated figure of people affected by AD in Spain is about 527,563, and for Andalusia, where this study was conducted, 83,205 people (data calculated from National Institute of Statistics. Population and Housing Census data, 2011).
The main risk factor for dementia is age. European society and particularly the Spanish, is aging.10,11 Therefore it is imperative to value the economic impact of pathologies linked with aging. These diseases are matters of concern for social policies and budgets within the European Union.12
Given the amount of potential cases and their costs we wondered about the existence of previous research regarding the direct (DC) and indirect costs (IC) assumed by the families. All costs that imply an out-of-pocket payment by the caregivers (home care services, materials necessary for care…) or by public services (medical consultations, social services, telecare, day-care units, nursing homes, etc) are considered as DC. All costs that do not imply a payment-out-of-pocket, but dedication time are considered as IC, if this time is not provided by a caregiver it would be provided by a professional. We value the time of caring (reduction of leisure and working time) as opportunity costs (OC).
We have conducted this research in the south of Spain (Andalusia) an area larger than Austria or Holland, and with a population higher than Finland or Ireland. The general population characteristics are in line with the general Spanish profile and Mediterranean cultures, where the family are the core careers.
In view of the epidemiological data previously referred to and after a bibliographic research, we found that there were no equivalent studies, neither in the geographical area, nor by size. We want to measure the different contribution of the State and families at each stage of severity. Consequently, we considered it of interest to do an empirical study to quantify the opportunity cost of the AD.
Our aim was to prove the following objectives: a) the costs of the illness increase with severity and the families assume more than 50% of these costs at each different stage,13–19 b) the costs are higher when the caregiver has a higher level of training, and when occupied, c) when the caregiver is male the costs are higher, and d) cohabiting reduces the DC of caring.
MethodThe sampling procedure was selective non-probabilistic sampling. The collection of data took place over six months, from January to June 2012, one of the researchers maintained weekly contact with those responsible for data collection.
Researchers contacted the Alzheimer's associations in Andalusia to ask for their collaboration. 32 demonstrated their interest in collaborating, but nine were rejected. Associations’ members were informed. Only those who were providing care when interviewed and gave consent participated. For ethical reasons, no personal data was collected. Participants could withdraw consent at any time.
Data was collected using a questionnaire specifically designed for the purpose. A trained interviewer was in charge of conducting the interview. Interviews took 15-20min to complete and were conducted at the Alzheimer's associations.
The estimated figure for people affected by dementia in Andalusia is 83,205.4,7,8,10 For a maximum error of 5%, the sample size needed for a confidence level of 99% would have been 665 people. Our sample was of 778 people. With this sample, our maximum error for a confidence level of 99% was 4.60%, and 3.50% for a confidence level of 95%.
To calculate the sample size, we use the equation:

To calculate the maximum error, we use the equation:
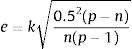
where n: sample size; k: constant (it takes the value 1.96 for a confidence level of 95%, and 2.58 for 99%); e: desired sample error (we choose 5%); p: people in the population with the desired characteristics (if unknown, p=q=0.5); and q: people in the population without the desired characteristics (q=1 − p). The costs are measured by the DC paid by the families (questionnaire data), by the contribution of the State (by transfers) and by concerted social services (we did not measure public health benefits). IC are measured by the reveal preferences method based on the OC, considering: a) the severity of the patient leads to b) different intensity of attention (time), and c) the level of education of the caregiver implies a higher time factor cost.
Direct private cost (DPC) is calculated as the sum of the annual cost due to: 1) Support services contracted to help the main caregiver, 2) In the case of institutionalised patients, the costs of the nursing home, and 3) other social-health costs related to the patient (such as legal or tracking services).
In the case of DC assumed by the State (DCS), when the services were totally or partially covered by the State, we subtracted the amount the family paid from the public cost. The amount assumed by the State is published in the Official Bulletin of the State or, in this case also, in the Official Bulletin of the Junta of Andalusia.
The severity of the stage was based on the Global Deterioration Scale (GDS) of Reisberg et al.20 GDS takes values from 1 (normality) to 7 (very severe dementia).
The weight of the hours dedicated to care taking is not linearly proposed because the evolution of the syndrome is not. The tendency among caregivers is to overestimate, when asked, the time they dedicate to care taking. To better weigh the hours of caring we followed a similar distribution of the intensity of time that was used by a previous study of the economic impact of the AD in Europe.21 For the intensity of time of caring we would attribute an average of: 2.4hours 10% of the day for mild levels (2 and 3 GDS), 8hours 1/3 of the day- for moderate (4 and 5 GDS), and 24hours for severe (6 and 7 GDS), 16hours valued as labour cost of caring, and 8hours, which make up 24, valued as leisure time.
In order to calculate average wages by educational level we took the figures published by the INE (Instituto Nacional de Estadística, Office for National Statistic).22 For 2012, the year of data collection, the gross wages were: 1,368.2 €, (primary level of education) 1,609.5 € (secondary), and 2,375.8 € (higher).
Where people did not study we considered a close approximation to reality to take the minimum wage in 2012, 641.6 € as a reference. In the case of retirees the OC of their time was estimated.23 The average pension was 858.4 €. We did not differentiate by educational level given that no data was available, and in most cases the large majority of the sample was of very similar level of training. The full time working day was taken as 40h/p/w (160h/p/m).
The evaluation of time dedicated by caregivers was calculated by training level and we also distinguished into two potential uses of time (T): working time (Wt) and leisure time (Lt). The total OC is the sum of the n subjects, considering the stages of the syndrome (we distinguished three: mild, moderate, and severe; j=1,2,3), and level of the caregiver's education (we distinguished three 3: primary, secondary and higher; k=1,2,3). The equation for the OC is:
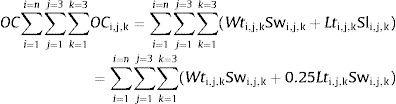
Considering: Slij=0.25Swij
And: Ltij=1−Wtij
where i: subject (i: 1,2,3…n); j: level of severity (mild, moderate, and severe; j: 1,2,3); k: level of education of the caregiver (k=1,2,3; 1: primary, 2: secondary, 3: higher); Sw: economic evaluation of working time (wages); and Sl: economic evaluation of leisure time (25% of Sw).
The value of leisure time is an estimation (25% of working time), and consequently subjective depending on age, type of job, previous work experience; in general it is agreed to be on average between 25% and 33% of the value of working time.23–26
In our evaluation of the OC we considered the following cases to estimate the time dedicated to caregiving and to leisure time, that changed based on the stage of the patient and working situation of the caregiver.
Where people are unoccupied all their hours are calculated as wages of leisure time (Sl), and in the case of retirees equally (in this case calculated according to the average pension).
To determine differences among the groups and to contrast the independence of qualitative vs quantitative variables we used the t-Student test for independent samples. For comparison of two or more groups we used the ANOVA (analysis of variance). We previously confirmed the cases of application: 1) normality, 2) homoscedasticity and 3) independency. For the cases with more than one dependent variable we used the MANOVA (multivariate analysis of variance). Data analysis was performed with the SPSS-22 Software.
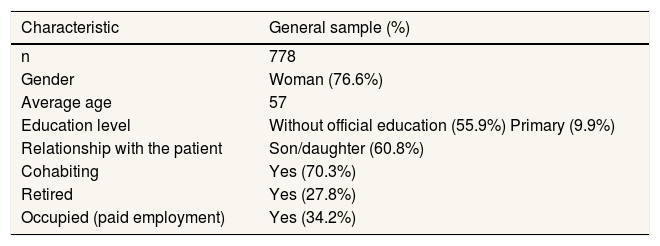
ResultsThe general profile of patient is that of a woman (71.3%), elderly, with a mean age of 79.53 (standard deviation: 7.49) years old. The most common type of dementia was AD, 83.2%. The main characteristics of caregivers are summarised in Table 1. By gender, the proportion of occupied caregivers is greater for males than females (37.9% vs 32.2%) and the education level is also higher for males. 43% of males have secondary or higher education, females only 31.4%
General profile of the sample of caregivers.
| Characteristic | General sample (%) |
|---|---|
| n | 778 |
| Gender | Woman (76.6%) |
| Average age | 57 |
| Education level | Without official education (55.9%) Primary (9.9%) |
| Relationship with the patient | Son/daughter (60.8%) |
| Cohabiting | Yes (70.3%) |
| Retired | Yes (27.8%) |
| Occupied (paid employment) | Yes (34.2%) |
As occupied caregivers, we consider those are not unemployed nor retired, and are in a paid employment. As cohabiting we consider those are living together for at least six months a year.
Source: compiled by the authors based on the data of the sample.
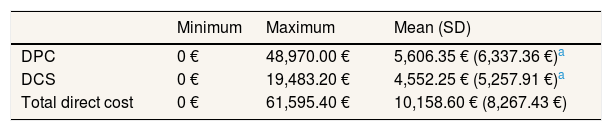
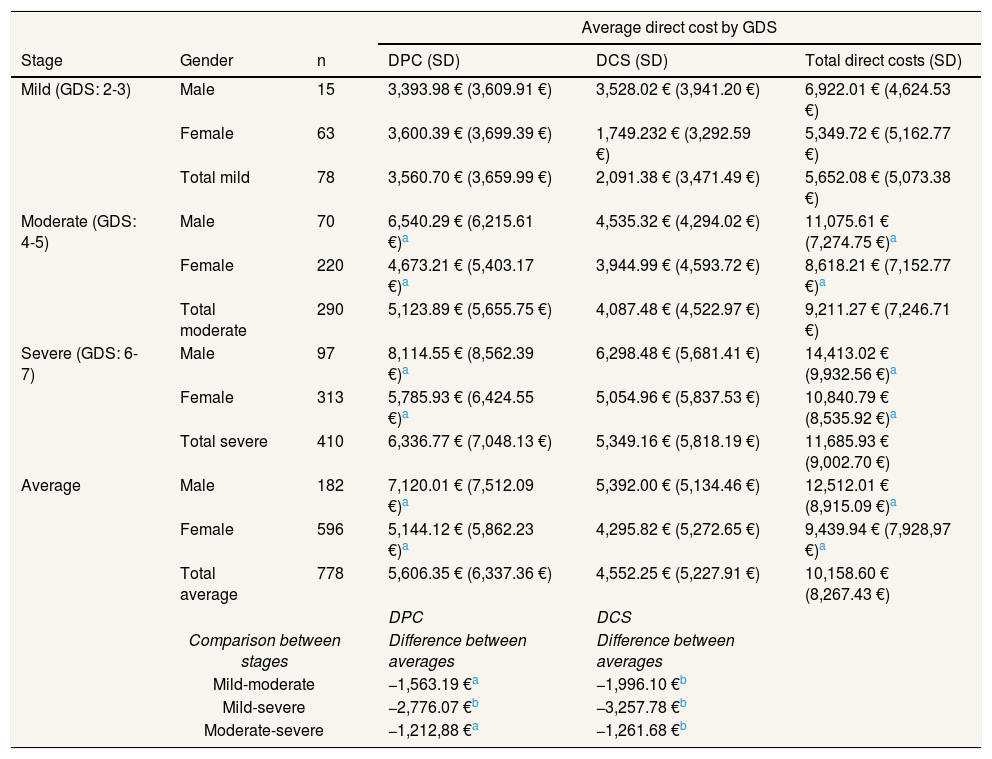
The DC show a broad variation in the sample, as can be seen on Table 2. The cost supported by the family, on average, is higher by 1,054.10 € (23.2%) than assumed by the State. However, to better judge the contribution of each it is convenient to value it according to the different stages of the syndrome, as can be seen on Table 3. In this table, we can appreciate that the costs increase with the level of severity. The average DPC range from 5,606.35 € (55.18%), to 48,970.00 € (79.50%).
Annual direct private cost (payments out-of-pocket of the families) vs direct cost assumed by the State.
| Minimum | Maximum | Mean (SD) | |
|---|---|---|---|
| DPC | 0 € | 48,970.00 € | 5,606.35 € (6,337.36 €)a |
| DCS | 0 € | 19,483.20 € | 4,552.25 € (5,257.91 €)a |
| Total direct cost | 0 € | 61,595.40 € | 10,158.60 € (8,267.43 €) |
DCS: direct cost for the State; DPC: direct private cost; SD: standard deviation.
Annual direct private costs (payments out-of-pocket of the families) vs. direct costs assumed by the State, by level of severity valued with the GDS and gender.
| Average direct cost by GDS | |||||
|---|---|---|---|---|---|
| Stage | Gender | n | DPC (SD) | DCS (SD) | Total direct costs (SD) |
| Mild (GDS: 2-3) | Male | 15 | 3,393.98 € (3,609.91 €) | 3,528.02 € (3,941.20 €) | 6,922.01 € (4,624.53 €) |
| Female | 63 | 3,600.39 € (3,699.39 €) | 1,749.232 € (3,292.59 €) | 5,349.72 € (5,162.77 €) | |
| Total mild | 78 | 3,560.70 € (3,659.99 €) | 2,091.38 € (3,471.49 €) | 5,652.08 € (5,073.38 €) | |
| Moderate (GDS: 4-5) | Male | 70 | 6,540.29 € (6,215.61 €)a | 4,535.32 € (4,294.02 €) | 11,075.61 € (7,274.75 €)a |
| Female | 220 | 4,673.21 € (5,403.17 €)a | 3,944.99 € (4,593.72 €) | 8,618.21 € (7,152.77 €)a | |
| Total moderate | 290 | 5,123.89 € (5,655.75 €) | 4,087.48 € (4,522.97 €) | 9,211.27 € (7,246.71 €) | |
| Severe (GDS: 6-7) | Male | 97 | 8,114.55 € (8,562.39 €)a | 6,298.48 € (5,681.41 €) | 14,413.02 € (9,932.56 €)a |
| Female | 313 | 5,785.93 € (6,424.55 €)a | 5,054.96 € (5,837.53 €) | 10,840.79 € (8,535.92 €)a | |
| Total severe | 410 | 6,336.77 € (7,048.13 €) | 5,349.16 € (5,818.19 €) | 11,685.93 € (9,002.70 €) | |
| Average | Male | 182 | 7,120.01 € (7,512.09 €)a | 5,392.00 € (5,134.46 €) | 12,512.01 € (8,915.09 €)a |
| Female | 596 | 5,144.12 € (5,862.23 €)a | 4,295.82 € (5,272.65 €) | 9,439.94 € (7,928,97 €)a | |
| Total average | 778 | 5,606.35 € (6,337.36 €) | 4,552.25 € (5,227.91 €) | 10,158.60 € (8,267.43 €) | |
| DPC | DCS | ||||
| Comparison between stages | Difference between averages | Difference between averages | |||
| Mild-moderate | −1,563.19 €a | −1,996.10 €b | |||
| Mild-severe | −2,776.07 €b | −3,257.78 €b | |||
| Moderate-severe | −1,212,88 €a | −1,261.68 €b | |||
DCS: direct cost for the State; DPC: direct private cost; GDS: Global Deterioration Scale; SD: standard deviation.
To ascertain if the differences in cost based on the level of severity were statistically significant (Table 3) we performed an ANOVA of one factor. There are significant differences between the 3 levels.
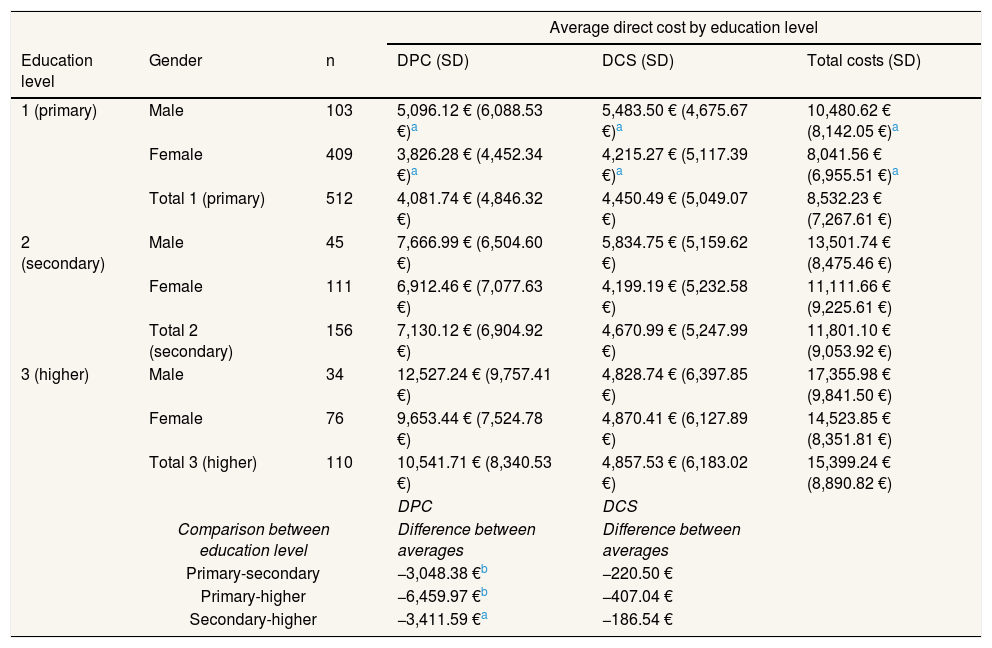
As seen on Table 4, we analysed the data again with a one factor ANOVA. The average DC clearly increases by educational level. DCS increase too, but there are no significant differences. Costs, especially the DPC, are higher if the caregiver is occupied. DCS are also higher for occupied caregivers, but the difference is only significant in the first case.
Direct costs by education level and by working situation of the main caregiver and gender.
| Average direct cost by education level | |||||
|---|---|---|---|---|---|
| Education level | Gender | n | DPC (SD) | DCS (SD) | Total costs (SD) |
| 1 (primary) | Male | 103 | 5,096.12 € (6,088.53 €)a | 5,483.50 € (4,675.67 €)a | 10,480.62 € (8,142.05 €)a |
| Female | 409 | 3,826.28 € (4,452.34 €)a | 4,215.27 € (5,117.39 €)a | 8,041.56 € (6,955.51 €)a | |
| Total 1 (primary) | 512 | 4,081.74 € (4,846.32 €) | 4,450.49 € (5,049.07 €) | 8,532.23 € (7,267.61 €) | |
| 2 (secondary) | Male | 45 | 7,666.99 € (6,504.60 €) | 5,834.75 € (5,159.62 €) | 13,501.74 € (8,475.46 €) |
| Female | 111 | 6,912.46 € (7,077.63 €) | 4,199.19 € (5,232.58 €) | 11,111.66 € (9,225.61 €) | |
| Total 2 (secondary) | 156 | 7,130.12 € (6,904.92 €) | 4,670.99 € (5,247.99 €) | 11,801.10 € (9,053.92 €) | |
| 3 (higher) | Male | 34 | 12,527.24 € (9,757.41 €) | 4,828.74 € (6,397.85 €) | 17,355.98 € (9,841.50 €) |
| Female | 76 | 9,653.44 € (7,524.78 €) | 4,870.41 € (6,127.89 €) | 14,523.85 € (8,351.81 €) | |
| Total 3 (higher) | 110 | 10,541.71 € (8,340.53 €) | 4,857.53 € (6,183.02 €) | 15,399.24 € (8,890.82 €) | |
| DPC | DCS | ||||
| Comparison between education level | Difference between averages | Difference between averages | |||
| Primary-secondary | −3,048.38 €b | −220.50 € | |||
| Primary-higher | −6,459.97 €b | −407.04 € | |||
| Secondary-higher | −3,411.59 €a | −186.54 € | |||
| Average direct cost by working situation | |||||
|---|---|---|---|---|---|
| Working situation | Gender | n | DPC (SD) | DCS (SD) | Total costs (SD) |
| 1 (occupied) | Male | 69 | 8,930.27 € (9,039.14 €)a | 6,210.79 € (5,484.69 €) | 15,141.06 € (9,163.68 €)a |
| Female | 192 | 6,667.23 € (6,934.07 €)a | 4,8073.04 € (5,379.91 €) | 11,540.27 € (8,640.04 €)a | |
| Total 1 (occupied) | 261 | 7,265.51 € (7,595.42 €) | 5,226.69 € (5,429.48 €) | 12,492.07 € (8,906.89 €) | |
| 2 (retired) | Male | 18 | 6,424.22 € (7,482.37 €) | 3,893.57 € (4,302.77 €) | 10,317.80 € (8,881.93 €) |
| Female | 283 | 4,555.80 € (5,477.28 €) | 3,964.02 € (5,395.79 €) | 8,519.81 € (7,769.83 €) | |
| Total 2 (retired) | 301 | 4,667.53 € (5,681.72 €) | 3,959.80 € (5,330.76 €) | 8,627.33 € (7,835.86 €) | |
| 3 (unoccupied) | Male | 95 | 5,937.01 € (5,959.57 €)a | 5,081.22 € (4,963.17 €) | 11,018.24 € (8,353.13 €)a |
| Female | 121 | 4,103.28 € (4,212.51 €)a | 4,155.93 € (4,748.23 €) | 8,259.21 € (6,369.77 €)a | |
| Total 3 (unoccupied) | 216 | 4,909.78 € (5,124.91 €) | 4,562.89 € (4,854.42 €) | 9,472.67 € (7,418.65 €) | |
| DPC | DCS | ||||
| Comparison between working situation | Difference between averages | Difference between averages | |||
| Occupied-retired | 2,597.98 €b | 1,266.89 €a | |||
| Occupied-unoccupied | 2,355.72 €b | 663.81 € | |||
| Retired-unoccupied | −242.25 € | −603.81 € | |||
DCS: direct cost for the State; DPC: direct private cost; SD: standard deviation.
For the comparison of DPC between genders (Table 5) we applied the t-Student test for independent samples. The differences in annual costs were significant between males and females, and the same occurred for total costs. The DPC are higher when the caregiver is male, the opposite occurred with the DCS in this case the difference is not significant.
Average direct costs assumed by the family (private costs) and by the State by gender and cohabiting or not.
| Average direct cost by sex of the main caregiver | ||||
|---|---|---|---|---|
| Gender of the caregiver | n | DPC (SD) | DCS (SD) | Total costs (SD) |
| Male | 182 | 7,120.00 € (7,512.09 €)a | 5,392.00 € (5,134.46 €) | 12,512.01 € (8,915.09 €)b |
| Female | 596 | 5,144.12 € (5,862.23 €)a | 4,295.82 € (5,272.65 €) | 9,439.94 € (7,928.97 €)b |
| Average direct cost by cohabiting situation | ||||
|---|---|---|---|---|
| Cohabiting | n | DPC (SD) | DCS (SD) | Total costs (SD) |
| Yes | 547 | 4,668.77 € (5,594.02 €)b) | 3,906.53 € (4,590.54 €)b | 8,575.30 € (7,303.51 €)b |
| No | 231 | 7,826.48 € (7,372.26 €)b | 6,081.31 € (6,326.84 €)b | 13,907.79 € (9,175.98 €)b |
DCS: direct cost for the State; DPC: direct private cost; SD: standard deviation.
Finally, we added the evaluation of cohabiting situation to the study (Table 5), to determine if it influenced the costs assumed by the family and the State. From the statistical descriptive we see the costs are influenced when not cohabiting. This tends to increase in all the modalities: DPC (3,157.71 €, 67.63%), DCS (2,174.78 €, 55.67%) and total (5,332.49 €, 62.18%). We applied the t-Student test for independent samples. The significance was high for the 3 types of costs. Thus, the non-cohabiting situation elevated the costs for the families (DPC) and for the State (DCS).
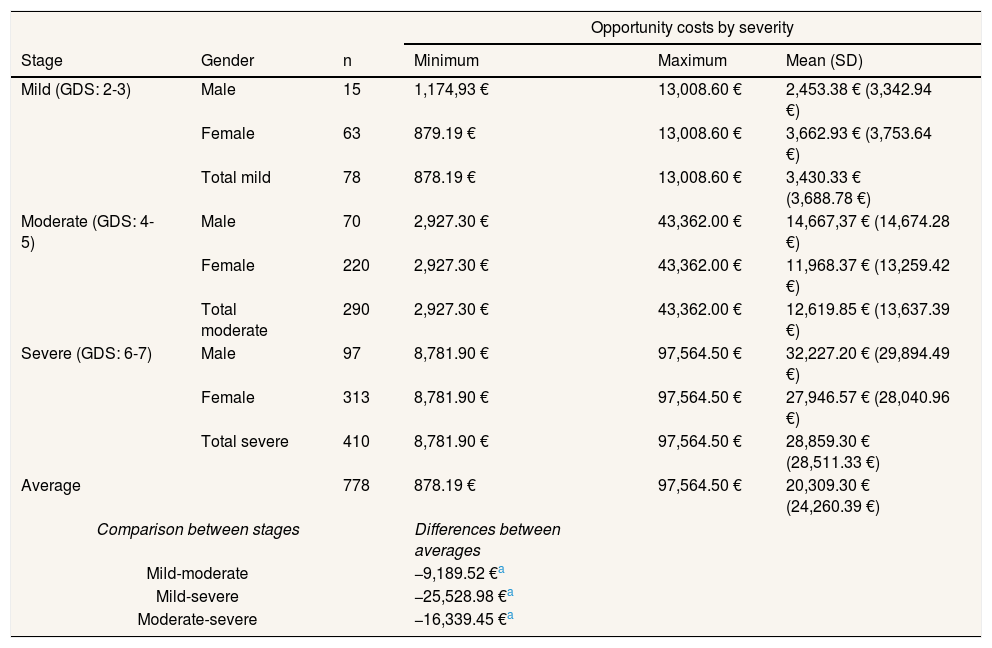
To determine the IC we proposed an analysis based on the calculation of the OC by the level of education of the caregiver and the patient's severity. OC grow (Table 6) with the level of education of the caregiver (the cost per hour is greater when the level of education is greater), and with the severity of syndrome (when the severity is higher the amount of attention needed is higher)
Average indirect costs for the caregivers by the severity of the syndrome, by education level and by gender calculated according to the opportunity costs model.
| Opportunity costs by severity | |||||
|---|---|---|---|---|---|
| Stage | Gender | n | Minimum | Maximum | Mean (SD) |
| Mild (GDS: 2-3) | Male | 15 | 1,174,93 € | 13,008.60 € | 2,453.38 € (3,342.94 €) |
| Female | 63 | 879.19 € | 13,008.60 € | 3,662.93 € (3,753.64 €) | |
| Total mild | 78 | 878.19 € | 13,008.60 € | 3,430.33 € (3,688.78 €) | |
| Moderate (GDS: 4-5) | Male | 70 | 2,927.30 € | 43,362.00 € | 14,667,37 € (14,674.28 €) |
| Female | 220 | 2,927.30 € | 43,362.00 € | 11,968.37 € (13,259.42 €) | |
| Total moderate | 290 | 2,927.30 € | 43,362.00 € | 12,619.85 € (13,637.39 €) | |
| Severe (GDS: 6-7) | Male | 97 | 8,781.90 € | 97,564.50 € | 32,227.20 € (29,894.49 €) |
| Female | 313 | 8,781.90 € | 97,564.50 € | 27,946.57 € (28,040.96 €) | |
| Total severe | 410 | 8,781.90 € | 97,564.50 € | 28,859.30 € (28,511.33 €) | |
| Average | 778 | 878.19 € | 97,564.50 € | 20,309.30 € (24,260.39 €) | |
| Comparison between stages | Differences between averages | ||||
| Mild-moderate | −9,189.52 €a | ||||
| Mild-severe | −25,528.98 €a | ||||
| Moderate-severe | −16,339.45 €a | ||||
| Opportunity costs by education level | |||||
|---|---|---|---|---|---|
| Education level | Gender | n | Minimum | Maximum | Mean (SD) |
| 1 (primary) | Male | 103 | 1,174.93 € | 56,173.50 € | 11,384.92 € (11,110.43 €) |
| Female | 409 | 878.19 € | 56,173.50 € | 9,900.81 € (8,920.99 €) | |
| Total primary | 512 | 878.19 € | 56,173.50 € | 10,199.37 € (9,409.43 €)) | |
| 2 (secondary) | Male | 45 | 1,174.94 € | 66,094.20 € | 34,694.10 € (26,070.42 €) |
| Female | 111 | 1,174.94 € | 66,094.20 € | 31,803.69 € (24,948.12 €) | |
| Total secondary | 156 | 1,174.94 € | 66,094.20 € | 32,637.46 € (25,226.43 €) | |
| 3 (higher) | Male | 34 | 1,174.94 € | 97,564.50 € | 42,813.94 € (36,666.07 €) |
| Female | 76 | 1,174.94 € | 97,564.50 € | 53,045.26 € (35,471.14 €) | |
| Total higher | 110 | 1,174.94 € | 97,564.50 € | 49,882.85 € (35,990.49 €) | |
| Comparison between education level | Differences between averages | ||||
| Primary-secondary | −22,438.09 €a | ||||
| Primary-higher | −39,683.48 €a | ||||
| Secondary-higher | −17,245.39 €a | ||||
GDS: Global Deterioration Scale; SD: standard deviation.
In this paper, we have developed an empirical study of the cost of the dementia in the Andalusian population. No other similar work has previously been performed regarding the relationship between the social costs of care for dementia patients and variables related to the socio-economic profile of the caregiver in Andalusia.
We have differentiated between DC and IC. The IC were valued with the revealed preferences method, based on the severity of the syndrome, some characteristics of the main caregiver (working situation or educational level) and other variables like gender, age of the caregiver, or cohabiting situation. We confirmed our objectives in all cases.
Scientific literature points to social costs being the best way to explain the costs of dementias, more than medical costs. These costs on average are under 5% of the total.27 McCarthy states that people with dementia consume few more resources than people with other illnesses.28 However, other studies underline the existence of comorbidities as a source of confusion when we read the costs.29
With the first objective, we chose to prove that the costs of the illness increase with severity and families assume more than 50% of these costs at each different stage. The results coincide generally with the literature.13,15,17,19
The DC of caring for patients lies mainly (more than 55%) with the family and by women.18 The role of the families indirectly means a considerable saving for the State that reduces their participation at the expense of families and patients themselves, but with a high OC, which is greater when the syndrome deteriorates.
When we observe the evolution of the DC related to the severity of the syndrome we appreciate that in the mild stages the amount funded by the families is much greater (63% of the total) than assumed by the State. In the mild stages patients are more autonomous and they need less care therefore the State provides less resources. Additionally, those people represent a smaller group in comparison to advanced stages, consequently most of the DC are supported by the families, but the average amount is smaller. The main contribution of caregivers is in terms of time of caring (an invisible contribution),30 not in payments out of pocket.
However, this apparent equality between public and private hides the reality. There is a “shadow cost” of this situation, which is the IC. As the syndrome evolves patients need more attention, however as we have shown the State hardly increases its economic resources in the more advanced stages. Therefore this increment of resources is provided by the families which means an additional cost to their health (psychologically and physically) shown in previous papers;31,32 and also an OC. DC therefore, hardly grow, but the IC for the families do exponentially.
The next objective we wanted to prove was that the costs are higher when caregivers have a higher level of training, and when they are occupied. The analysed data, for DC and IC, confirmed this objective.
Occupied people have a higher level of income, which facilitates a higher level of expenditure, and they need external support for their sick relative while working. This data proved interesting because if the level of education is higher and employment situation is occupied, more services will be contracted and more employment in the care sector will be generated. Policymakers should consider this. The second objective concerning the link between employment and level of education with the DC and IC is confirmed.
Another issue that we proposed was the relationship between caregiverś gender and costs. In the case of males, the tendency to care for others is more residual than in females. Additionally, the employment rate and the level of education are higher in males. These characteristics lead them more commonly to seek external support when they have to, so the cost is greater. When the caregiver is male it is more common that the patient is a partner (similar elevated age), meanwhile in the general group it is usually the daughter, who contracts external support. This explains why when the caregiver is male the costs are higher. The objective was confirmed.
Most of care is provided at home. Cultural reasons and socio-economic circumstances could explain these preferences. We therefore posed the question as to whether cohabiting with the patient affected the payment-out-of-pocket of the families. We proposed that the need for external care would be less if the caregiver cohabited due to less need for external support in these cases. Effectively this objective was corroborated. The provision of care by those that live in the same house reduces not only the DPC, but also the DCS and the total.
One aspect that should be analysed more profoundly in future studies is that of the generational gap between caregivers. Currently, as was proved, the average profile of caregiver is that of a low educational and occupational level, among others. The profile of new generations is plainly different which has multiple consequences. The OC are linked to occupational situation and academic level. Consequently, when the average level increases so does this type of cost. This must be considered for social policies for future generations, as the academic level of the younger generation is higher than that of current caregivers.
The costs of dementias are very high. A paper proposed that costs in Spain are comparatively higher than in other European countries due to its cost structure.33 It would be interesting for future lines of research to add the replacement costs, or to run this analysis at a national level. It would also be interesting to study the impact that deceleration of the syndrome would have. If new treatment plans prove successful in the stages with less economic impact it would lead to a new distribution of cost and less patients in the advanced stages of AD.34,35 Policymakers could examine budgetary allocations for research. At-risk population increases mean dedicating more funds to social and health policies will be needed.
Most of the care is provided at home and women are the main caregivers of people with Alzheimer's. The people with Alzheimer's is increasing. However, no study has ever been done to know the of in terms of costs for caregivers of a region that represent 17% of the total the population of Spain.
What does this study add to the literature?This study adds information about the direct and indirect cost of caregiver from southern Spain, and which are the main drivers of them. We have measure the different contribution in each stage of severity of the State and families.
David Cantarero.
Transparency declarationThe corresponding author on behalf of the other authors guarantee the accuracy, transparency and honesty of the data and information contained in the study, that no relevant information has been omitted and that all discrepancies between authors have been adequately resolved and described.
Authorship contributionsManuel Ruiz-Adame Reina was responsible of the data collection, designed the methodology of the study and performed the data analyses. Ruiz-Adame Reina, Correa and Burton have participated in the writing of the manuscript. All authors have done a supervision and review of the manuscript
FundingNone.
Conflicts of interestsNone.
The authors wish to thank the Alzheimer's Association of Andalusia, and especially to the Asociación Alzheimer Santa Elena (Seville), for their collaboration and encouragement to do this research. We also want to thank Prof. Carmen González Camacho, Dep. Applied Economics III, Univ. of Seville, for her help with the design of the research and advice. Finally, authors want to thank to the Research Group SEJ-393: Public Economy and Globalization for their support.











