



To explore the moderating and mediating role(s) of learning within the relationship between sense of coherence (SOC) and generalized resistance resources.
MethodCross-sectional study (N=481), using a self-administered questionnaire, of employees working in the healthcare sector in the Netherlands in 2017. Four residential healthcare settings and one healthcare-related Facebook group were involved. Multiple linear regression models were used to test for moderating and mediating effects of learning.
ResultsSocial relations, task significance, and job control significantly explained variance in SOC. Conceptual, social, and instrumental learning, combined, moderated the relationship between SOC and task significance. Instrumental learning moderated the relationship between job control and SOC. Social learning also mediated this relationship. Conceptual learning did not show any moderating or mediating effect.
ConclusionsThe relationship between SOC and the three GRRs seems to be strengthened or explained−to a certain extent−by instrumental and social learning. Healthcare organizations are recommended to promote learning through formal activities as well as through cooperation, feedback, sharing experiences, and job challenges. This requires employee participation and a multilevel interdisciplinary approach.
Explorar el rol del aprendizaje conceptual, instrumental y social en la relación entre el sentido de la coherencia (SC) y los recursos generales de resistencia (RGR) clave.
MétodosSe realizó un estudio transversal en 2017 (N=481) a profesionales del sector sanitario en Holanda mediante un cuestionario autoadministrado. Participaron cuatro centros de residencia geriátrica, así como un grupo de profesionales de salud de la red social de Facebook. Se utilizaron modelos de regresión lineal múltiple para evaluar los efectos de los roles de moderación y mediación del aprendizaje.
ResultadosLas relaciones sociales, el significado de las tareas y el control del trabajo explicaron de manera significativa la varianza en el SC. La combinación del aprendizaje conceptual, instrumental y social moderó la relación entre el SC y el significado de las tareas. El aprendizaje instrumental moderó la relación entre el control del trabajo y el SC. El aprendizaje social también medió en esta relación. Sin embargo, el aprendizaje conceptual no mostró ningún efecto moderador ni mediador.
ConclusionesLa relación entre el SC y estos tres RGR parece verse fortalecida o explicada, en cierta medida, por el aprendizaje instrumental y social. Se recomienda a las organizaciones sanitarias promover el aprendizaje a través de actividades formales, así como mediante la cooperación, comentarios, intercambio de experiencias y desafíos laborales. Esto requiere la participación del profesional, así como una cooperación multidisciplinaria y a distintos niveles.
In present-day society, organizations are challenged to inspire and empower employees to apply their full capabilities and should ensure that working conditions include resources that will motivate and energize them.1 Accordingly, employees are expected to show initiative and to be innovative and psychologically connected to their jobs.2 Job tasks and thus job characteristics are shifting from primarily physical to psychosocial work processes; this means that physical health and workability are not sufficient prerequisites to fulfil such jobs.3 Healthcare workers, particularly nurses and caregivers, are frequently exposed to psychosocial work-related factors, for instance, work overload. These factors are related to the development of adverse health and wellbeing, which in turn affect the functionality of nursing profession and the quality of care provided.4 Therefore, it is important to ensure that their work makes a positive contribution to their health and wellbeing.5 In this vein, workplace health means that healthcare workers should have the ability to participate and be productive in a sustainable and meaningful way.6
The focus on organizational flaws and individual shortcomings, known as the pathogenic approach, is not enough to strengthen this ability.3,7 This approach can be complemented by emphasizing organizational as well as individual conditions, resources, and determinants that create health and wellbeing at work; this is known as the salutogenic approach.8 Within salutogenic theory, two key concepts are central: sense of coherence (SOC) and generalized resistance resources (GRRs).9,10
SOC is defined as “a global orientation that expresses the extent to which one has a pervasive, enduring though dynamic feeling of confidence that (1) the stimuli deriving from one's internal and external environments in the course of living are structured, predictable, and explicable; (2) the resources are available to one to meet the demands posed by these stimuli; and (3) these demands are challenges, worthy of investment and engagement”.9 Employees with a strong SOC feel confident that resources are available to cope with work demands and are more likely to select an appropriate coping strategy.8 These resources are the GRRs, which give the prerequisites for the development of SOC.8 SOC increases with age and is strongly related to a variety of employee health and wellbeing outcomes.8,11 For instance, employees with a strong SOC show less psychosomatic symptoms and emotional exhaustion than employees with a weak SOC.7 GRRs can be found within people as resources bound to their person and capacity, but also to their physical and social work environment.8 In workplaces, social relations, task significance, and job control are key GRRs.6
“Job control” is defined as job and organizational characteristics such as employees’ decision-making authority, opportunities to use skills and knowledge, and opportunities to participate.12 It involves employees’ authority to make decisions concerning their jobs and the use of skills regarding task variety and options to develop and learn new things.13 “Social relations” is defined as the extent to which individuals can count on information, assistance, and appreciation from their colleagues at work.14 Social support concerns the frequency of opportunities to get help from direct colleagues and managers, as well as the frequency of situations where colleagues are willing to listen and reflect.6 “Task significance” is defined as the perception that one's job has a positive impact on other people.15 It is linked to a positive congruence between work activities and personal values, accompanied by strong feelings of identification with the attitudes, values, or goals of the working tasks and a sense of motivation and involvement.16,17
Vaandrager and Koelen6 developed a model in which SOC is assumed to have a relationship with the GRRs social relations, task significance, and job control. Over time, SOC and GRRs predict and strengthen each other, suggesting a dynamic and reciprocal relationship.2 GRRs strengthen the ability of employees to view life (work) as comprehensible, manageable, and meaningful, which in turn could influence the levels of perceptual, appraisal, and behaviour processes that strengthen their GRRs.2 However, the GRRs central in this study have not been tested in relation to SOC before, and the processes underlying the development of SOC are little understood.18
In salutogenic theory, developing health and wellbeing is a lifelong learning process in which people identify their GRRs, within themselves or in their immediate environment, thereby fostering sets of life experiences that strengthen their SOC.19 Workplace learning is part of this lifelong learning process, which has been assumed to be a key mechanism for building SOC and GRRs in workplaces.6 Healthcare workers are expected to develop themselves continuously to a fast-changing work environment,20 not only through education and training but also through engagement in daily work-related activities.21 Therefore, it can be hypothesized that learning at work could affect the relationship between SOC and GRRs,6 by either strengthening (moderating) or explaining (mediating) this relationship.
These ongoing learning processes in workplaces can be disentangled into three concepts: conceptual, instrumental, and social learning.20–24 Conceptual learning encompasses acquiring knowledge through the autonomous conception of new ideas, through moments of reflection on a sum of experiences, and through thinking about work behaviour.24,25 Instrumental learning encompasses the development of skills through formal activities like following courses or through learning on the job.24,26 Social learning entails learning from other people in the workplace through cooperation, feedback, sharing experiences, but also through job challenges like the growth of responsibilities or changes in tasks and functions.24,27
The present study aims to explore the moderating and mediating roles learning may have within the relationship between SOC on the one hand and social relations, task significance, and job control on the other hand. Examining the role of learning could provide insights into key learning processes that can be used to build SOC and GRRs in workplaces.3,6 The following three hypotheses are formulated to test whether SOC and GRRs have a positive relationship with each other and whether learning strengthens or explains this relationship:Hypothesis 1 Each of the three GRRs has a positive partial correlation with SOC after correcting for the other two. Learning moderates the relationship between SOC and GRRs. Learning mediates the relationship between SOC and GRRs.
A cross-sectional design was used.28 The study population consisted of Dutch nurses and caregivers employed in residential healthcare settings. Current estimates show that approximately 177.000 people are employed as nurses or caregivers, of which 25% work in residential healthcare settings.29 The majority is aged between 50-60 years, and more women (25%) work in this sector than men (12.2%).29
The sampling frame consisted of nurses and caregivers working in residential healthcare settings. Four healthcare settings from different institutions in the northern part of the Netherlands were involved (see Acknowledgements). Also, one healthcare-related Dutch Facebook group was included. This online community is mainly for nurses and caregivers working in residential healthcare settings and hospitals.
MeasurementsData collection was carried out in March and April 2017 by means of a self-administered questionnaire. Qualtrics software was used to develop the online version. A meta-analysis of techniques to improve participation rates in surveys amongst healthcare workers showed that a response rate of at least 38% could be expected for an online questionnaire.30 The questionnaire contained a variety of subscales measuring SOC, GRRs, learning, and demographic data.
SOCThe SOC concept has been shown to be well applicable in workplaces.7 SOC was measured by using the Dutch version (13 items) of the Orientation to Life Questionnaire,31 which has been shown to be valid and reliable, with a Cronbach's alpha of 0.89.32
GRRsThe three GRRs were measured using subscales from two validated questionnaires, namely, the Knowledge Intensive Working Environment Survey Target (KIWEST)29 and the Copenhagen Psychosocial Questionnaire II (COPSOQ II).30 Both questionnaires assess a broad range of psychosocial work factors and are not attached to one specific theory or model.29,30 Moreover, the KIWEST, as well as the COPSOQ II, contain subscales that measure the three GRRs central to this study: social relations, task significance, and job control.
The KIWEST has been shown to have good convergent validity and internal validity.33 Recently, the Dutch version of the KIWEST was assessed for internal consistency, which has also shown to be good (Cornelissen, 2017, personal communication). The COPSOQ II has proved to have strong criteria validity, and the reproducibility of the Dutch version has been demonstrated to be good.34,35 Subscales and Cronbach's alpha (α) of the Dutch version of these two questionnaires were used to measure the three GRRs.
For the GRRs social relations, the following subscales were chosen as indicators: social support from supervisors (3 items; α=0.85); social support from colleagues (3 items; α=0.70); rewards (3 items; α=0.84); and social community at work (3 items; α=0.63). For the GRRs task significance, the subscale meaning of work (3 items; α=0.85) was chosen as an indicator. For the GRRs job control, the following subscales were chosen as indicators: influence on work (4 items; α=0.59); possibilities for development (4 items; α=0.84); job autonomy (4 items; α=0.74); and illegitimate tasks (4 items; α=0.73). In line with others,2 the different subscales were combined into three latent variables.
LearningLearning was measured by using the Workplace Learning Processes Questionnaire (WLPQ), which aims to measure conceptual, instrumental, and social learning.20–23 The WLPQ was translated from English into Dutch and pilot tested.
The WLPQ consists of three subscales representing the three learning concepts: conceptual (6 items), instrumental (6 items), and social learning (4 items). All items were measured on a five-point Likert scale (e.g. ‘taking initiative at work’ was scored from 1=never to 5=daily).
Demographic variablesThe variables sex, age, level of education, type of contract, and average number of hours worked per week were also measured.
Data analysisThe data were analysed using the statistical package IBM SPSS Statistics 24 and the SPSS add-on PROCESS36 for Windows. The level of significance was set at the recommended .05 level.37
Differences among the organizations regarding sex, level of education, type of contract, and response rates were tested using the Chi-square test. The Kruskal-Wallis H Test, one-way ANOVA, and an independent t-test were used to test for differences regarding age, average hours worked per week, and SOC.
Exploratory factor analysis was performed on the WLPQ items using its three underlying sub-constructs. A preliminary analysis was performed to examine the factorability of the 16 items by checking multicollinearity (determinant>0.00001), the KMO measure of sampling adequacy (>0.5), and the Bartlett's test of sphericity (p<0.05).37 Finally, a scree plot and eigenvalues>1 were used to assess the number of factors to extract.37
Correlation and reliability analyses (Cronbach's alpha) were used for all the study variables. Missing values were excluded by convention pairwise and listwise.37 Multiple linear regression analysis was performed to test whether the three GRRs explain variance in SOC with forced entry.37 This regression analysis was also used to test for moderating effects, after creating centred interaction terms between the predictor(s) (SOC or GRRs) and learning, using hierarchical entry.37 For instance, when testing for the moderating effects of learning on the relationship between SOC and its predictors, GRRs, the interaction terms between learning and the GRRs (e.g. job control * social learning) were added as predictor variables in the regression analysis. Moderating effects were explored by testing the significance of the additional explained variation of the dependent variable(s) (SOC or GRRs) when these interaction terms were added to the model, both individually and in groups. All regression analyses excluded missing values by convention listwise.37
Model 4 (simple mediation) from the add-on PROCESS function was used to examine indirect effects of learning,36 which means that the relationship between the dependent (e.g. SOC) and independent (e.g. job control) variable goes through another mediating variable (e.g. instrumental learning). Simple mediation allows adding one mediator (e.g. instrumental learning) to the regression model at a time, which is a conventional model used for exploring mediating effects.36 The significance of the mediation effect was studied using 10,000 bootstrapped samples, with a random seed number of 5,235.36 Since research showed that SOC increases with age,8 age was included in all regression analyses to control for possible confounding effects.
Ethical considerationsThis study was conducted according to the Wageningen Code of Conduct for Scientific Practice. Participation was entirely voluntary, sustained by an informed consent to ensure anonymity without using any incentives.
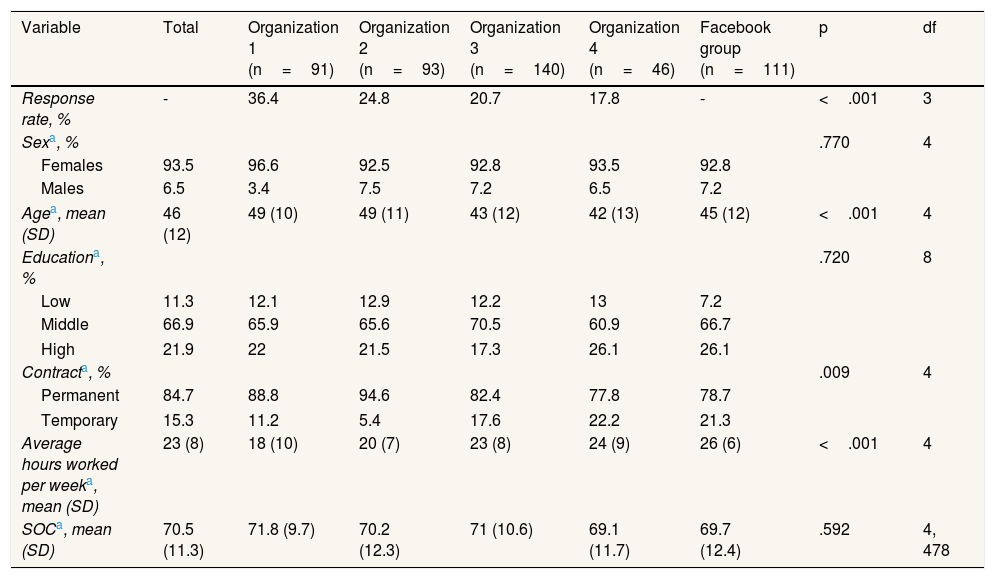
ResultsParticipantsTable 1 provides a summary of the demographic data for each of the five groups, including mean SOC and response rates. All response rates were lower than the anticipated 38%, and these rates differed significantly among the four healthcare groups, χ2(3)=47,80, p <0.001. Significant differences were also found regarding age, H(4)=25.82, p <0.001; average number of hours worked per week, H(4)=45.80, p <0.001; and type of contract, χ2(4)=13.45, p=0.009. SOC did not differ significantly among the five groups or between men (M=71.9, SD=12.7) and women (M=70.5, SD=11.2), t(473)=0.653. Since SOC did not significantly differ among the five groups, it was deemed appropriate to combine the five groups into a single dataset for testing the study hypotheses without stratifying, for instance, for sex. This is also in line with the overarching aim of this study, which is to test the model, and not invariances across specified subgroups.
Descriptive statistics and exploring differences among the five groups (N=481).
| Variable | Total | Organization 1 (n=91) | Organization 2 (n=93) | Organization 3 (n=140) | Organization 4 (n=46) | Facebook group (n=111) | p | df |
|---|---|---|---|---|---|---|---|---|
| Response rate, % | - | 36.4 | 24.8 | 20.7 | 17.8 | - | <.001 | 3 |
| Sexa, % | .770 | 4 | ||||||
| Females | 93.5 | 96.6 | 92.5 | 92.8 | 93.5 | 92.8 | ||
| Males | 6.5 | 3.4 | 7.5 | 7.2 | 6.5 | 7.2 | ||
| Agea, mean (SD) | 46 (12) | 49 (10) | 49 (11) | 43 (12) | 42 (13) | 45 (12) | <.001 | 4 |
| Educationa, % | .720 | 8 | ||||||
| Low | 11.3 | 12.1 | 12.9 | 12.2 | 13 | 7.2 | ||
| Middle | 66.9 | 65.9 | 65.6 | 70.5 | 60.9 | 66.7 | ||
| High | 21.9 | 22 | 21.5 | 17.3 | 26.1 | 26.1 | ||
| Contracta, % | .009 | 4 | ||||||
| Permanent | 84.7 | 88.8 | 94.6 | 82.4 | 77.8 | 78.7 | ||
| Temporary | 15.3 | 11.2 | 5.4 | 17.6 | 22.2 | 21.3 | ||
| Average hours worked per weeka, mean (SD) | 23 (8) | 18 (10) | 20 (7) | 23 (8) | 24 (9) | 26 (6) | <.001 | 4 |
| SOCa, mean (SD) | 70.5 (11.3) | 71.8 (9.7) | 70.2 (12.3) | 71 (10.6) | 69.1 (11.7) | 69.7 (12.4) | .592 | 4, 478 |
SD: standard deviation; SOC: sense of coherence.
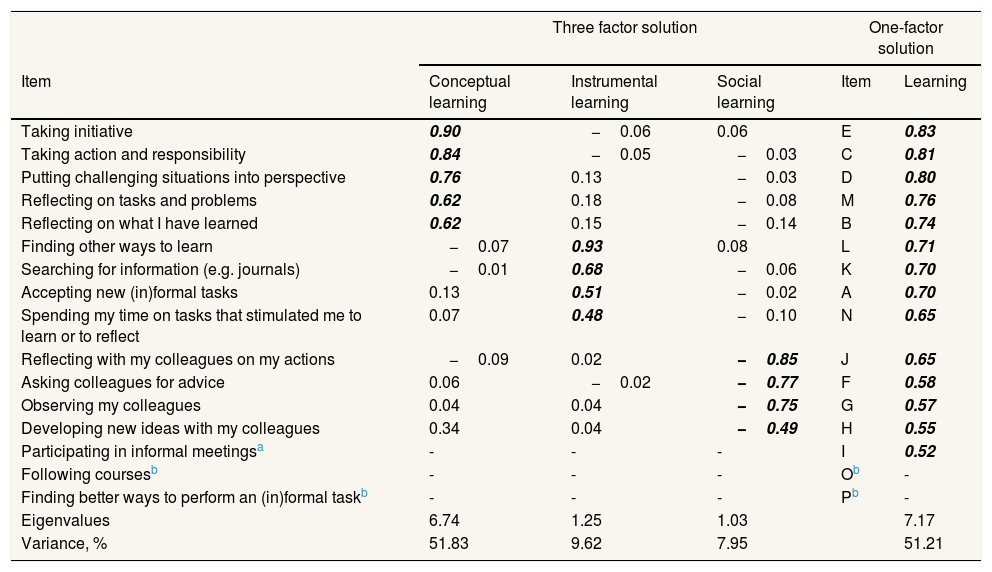
Principal axis factoring analysis was conducted with oblique rotation on the 16 items of the WLPQ (Table 2). Three factors had eigenvalues over Kaiser's criterion of 1 and in combination explained 69.40% of the variance. The scree plot, however, suggested both a three-factor solution and a one-factor solution. The one-factor solution explained 51.21% of the variance. Both the three-factor solution and the one-factor solution were retained.
Summary of two exploratory factor analysis results for the Workplace Learning Processes Questionnaire (N=481).
| Three factor solution | One-factor solution | ||||
|---|---|---|---|---|---|
| Item | Conceptual learning | Instrumental learning | Social learning | Item | Learning |
| Taking initiative | 0.90 | −0.06 | 0.06 | E | 0.83 |
| Taking action and responsibility | 0.84 | −0.05 | −0.03 | C | 0.81 |
| Putting challenging situations into perspective | 0.76 | 0.13 | −0.03 | D | 0.80 |
| Reflecting on tasks and problems | 0.62 | 0.18 | −0.08 | M | 0.76 |
| Reflecting on what I have learned | 0.62 | 0.15 | −0.14 | B | 0.74 |
| Finding other ways to learn | −0.07 | 0.93 | 0.08 | L | 0.71 |
| Searching for information (e.g. journals) | −0.01 | 0.68 | −0.06 | K | 0.70 |
| Accepting new (in)formal tasks | 0.13 | 0.51 | −0.02 | A | 0.70 |
| Spending my time on tasks that stimulated me to learn or to reflect | 0.07 | 0.48 | −0.10 | N | 0.65 |
| Reflecting with my colleagues on my actions | −0.09 | 0.02 | −0.85 | J | 0.65 |
| Asking colleagues for advice | 0.06 | −0.02 | −0.77 | F | 0.58 |
| Observing my colleagues | 0.04 | 0.04 | −0.75 | G | 0.57 |
| Developing new ideas with my colleagues | 0.34 | 0.04 | −0.49 | H | 0.55 |
| Participating in informal meetingsa | - | - | - | I | 0.52 |
| Following coursesb | - | - | - | Ob | - |
| Finding better ways to perform an (in)formal taskb | - | - | - | Pb | - |
| Eigenvalues | 6.74 | 1.25 | 1.03 | 7.17 | |
| Variance, % | 51.83 | 9.62 | 7.95 | 51.21 | |
Factor loadings over 0.40 appear in italics. Extraction: principal axis factoring with oblique rotation.
Regarding the three-factor solution: the items that cluster on the same factors suggest that factor 1 represents conceptual learning, factor 2 represents instrumental learning, and factor 3 represents social learning. The one-factor solution combined these three sub-constructs into a single latent variable designated as learning.
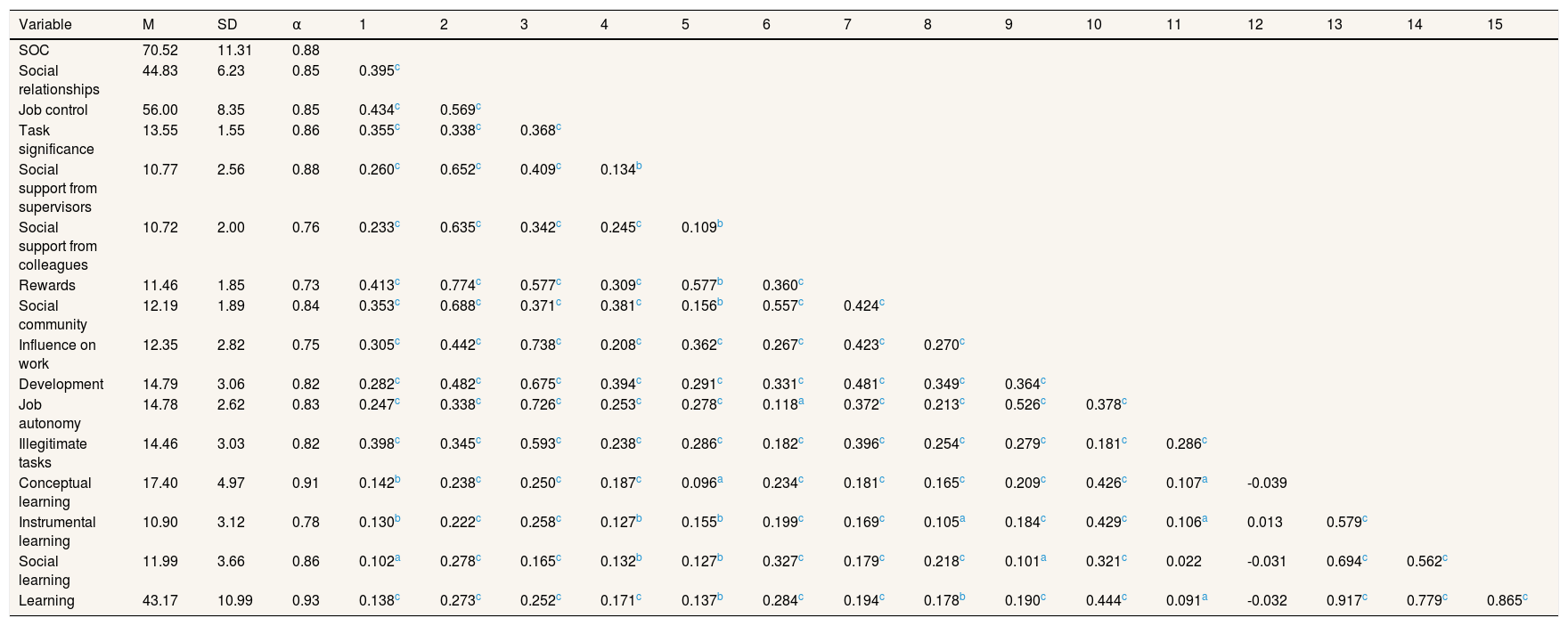
Table 3 displays the means, standard deviations, Cronbach's alphas, and correlations among the study variables. The Cronbach's alphas are good for all the study variables. SOC, the GRRs, and both factor solutions are positively correlated with one another.
Means (M), standard deviations (SD), internal consistencies (Cronbach's α), and correlations between the study variables (N=481).
| Variable | M | SD | α | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | 13 | 14 | 15 |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| SOC | 70.52 | 11.31 | 0.88 | |||||||||||||||
| Social relationships | 44.83 | 6.23 | 0.85 | 0.395c | ||||||||||||||
| Job control | 56.00 | 8.35 | 0.85 | 0.434c | 0.569c | |||||||||||||
| Task significance | 13.55 | 1.55 | 0.86 | 0.355c | 0.338c | 0.368c | ||||||||||||
| Social support from supervisors | 10.77 | 2.56 | 0.88 | 0.260c | 0.652c | 0.409c | 0.134b | |||||||||||
| Social support from colleagues | 10.72 | 2.00 | 0.76 | 0.233c | 0.635c | 0.342c | 0.245c | 0.109b | ||||||||||
| Rewards | 11.46 | 1.85 | 0.73 | 0.413c | 0.774c | 0.577c | 0.309c | 0.577b | 0.360c | |||||||||
| Social community | 12.19 | 1.89 | 0.84 | 0.353c | 0.688c | 0.371c | 0.381c | 0.156b | 0.557c | 0.424c | ||||||||
| Influence on work | 12.35 | 2.82 | 0.75 | 0.305c | 0.442c | 0.738c | 0.208c | 0.362c | 0.267c | 0.423c | 0.270c | |||||||
| Development | 14.79 | 3.06 | 0.82 | 0.282c | 0.482c | 0.675c | 0.394c | 0.291c | 0.331c | 0.481c | 0.349c | 0.364c | ||||||
| Job autonomy | 14.78 | 2.62 | 0.83 | 0.247c | 0.338c | 0.726c | 0.253c | 0.278c | 0.118a | 0.372c | 0.213c | 0.526c | 0.378c | |||||
| Illegitimate tasks | 14.46 | 3.03 | 0.82 | 0.398c | 0.345c | 0.593c | 0.238c | 0.286c | 0.182c | 0.396c | 0.254c | 0.279c | 0.181c | 0.286c | ||||
| Conceptual learning | 17.40 | 4.97 | 0.91 | 0.142b | 0.238c | 0.250c | 0.187c | 0.096a | 0.234c | 0.181c | 0.165c | 0.209c | 0.426c | 0.107a | -0.039 | |||
| Instrumental learning | 10.90 | 3.12 | 0.78 | 0.130b | 0.222c | 0.258c | 0.127b | 0.155b | 0.199c | 0.169c | 0.105a | 0.184c | 0.429c | 0.106a | 0.013 | 0.579c | ||
| Social learning | 11.99 | 3.66 | 0.86 | 0.102a | 0.278c | 0.165c | 0.132b | 0.127b | 0.327c | 0.179c | 0.218c | 0.101a | 0.321c | 0.022 | -0.031 | 0.694c | 0.562c | |
| Learning | 43.17 | 10.99 | 0.93 | 0.138c | 0.273c | 0.252c | 0.171c | 0.137b | 0.284c | 0.194c | 0.178b | 0.190c | 0.444c | 0.091a | -0.032 | 0.917c | 0.779c | 0.865c |
SOC: sense of coherence.
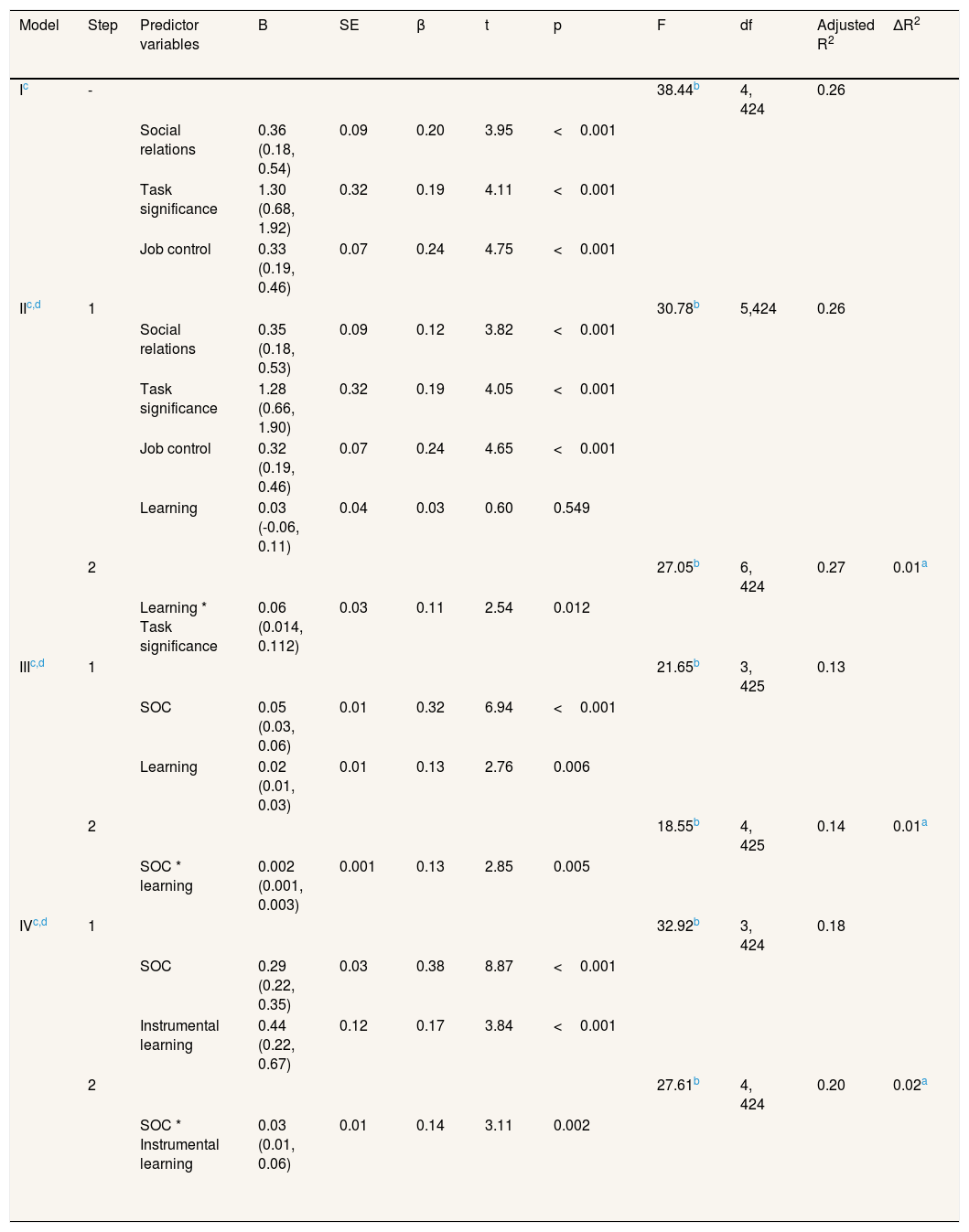
Table 4 presents the regression analysis for testing the relationship between SOC and the GRRs (model I), which shows how much variance is explained in SOC by the three GRRs. The three GRRs explain 26% (adjusted R2) of the variance very significantly in SOC. Moreover, each of the three GRRs contributes very significantly after correcting for the other two GRRs and age. Job control seems to be the most important GRRs (standardized β=0.24, p <0.001), followed by social relations (standardized β=0.20, p <0.001), and task significance (standardized β=0.19, p <0.001), thereby supporting hypothesis 1.
Linear models of the predictors of SOC, task significance, and job control.
| Model | Step | Predictor variables | B | SE | β | t | p | F | df | Adjusted R2 | ΔR2 |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Ic | - | 38.44b | 4, 424 | 0.26 | |||||||
| Social relations | 0.36 (0.18, 0.54) | 0.09 | 0.20 | 3.95 | <0.001 | ||||||
| Task significance | 1.30 (0.68, 1.92) | 0.32 | 0.19 | 4.11 | <0.001 | ||||||
| Job control | 0.33 (0.19, 0.46) | 0.07 | 0.24 | 4.75 | <0.001 | ||||||
| IIc,d | 1 | 30.78b | 5,424 | 0.26 | |||||||
| Social relations | 0.35 (0.18, 0.53) | 0.09 | 0.12 | 3.82 | <0.001 | ||||||
| Task significance | 1.28 (0.66, 1.90) | 0.32 | 0.19 | 4.05 | <0.001 | ||||||
| Job control | 0.32 (0.19, 0.46) | 0.07 | 0.24 | 4.65 | <0.001 | ||||||
| Learning | 0.03 (-0.06, 0.11) | 0.04 | 0.03 | 0.60 | 0.549 | ||||||
| 2 | 27.05b | 6, 424 | 0.27 | 0.01a | |||||||
| Learning * Task significance | 0.06 (0.014, 0.112) | 0.03 | 0.11 | 2.54 | 0.012 | ||||||
| IIIc,d | 1 | 21.65b | 3, 425 | 0.13 | |||||||
| SOC | 0.05 (0.03, 0.06) | 0.01 | 0.32 | 6.94 | <0.001 | ||||||
| Learning | 0.02 (0.01, 0.03) | 0.01 | 0.13 | 2.76 | 0.006 | ||||||
| 2 | 18.55b | 4, 425 | 0.14 | 0.01a | |||||||
| SOC * learning | 0.002 (0.001, 0.003) | 0.001 | 0.13 | 2.85 | 0.005 | ||||||
| IVc,d | 1 | 32.92b | 3, 424 | 0.18 | |||||||
| SOC | 0.29 (0.22, 0.35) | 0.03 | 0.38 | 8.87 | <0.001 | ||||||
| Instrumental learning | 0.44 (0.22, 0.67) | 0.12 | 0.17 | 3.84 | <0.001 | ||||||
| 2 | 27.61b | 4, 424 | 0.20 | 0.02a | |||||||
| SOC * Instrumental learning | 0.03 (0.01, 0.06) | 0.01 | 0.14 | 3.11 | 0.002 | ||||||
b: unstandardized regression coefficient; SE: standard error; β: standardized regression coefficient; t: obtained t-value; p: probability; F: obtained F-value; df: degrees of freedom; R2: proportion variance explained; ΔR2: increase in explained variance due to the moderation effect; Model I & II: dependent variable=SOC; Model III: dependent variable task significance; Model IV: dependent variable job control.
Table 4 also shows the moderation analyses (models II, III, and IV). The interaction term(s) between learning and predictor(s) (GRRs or SOC) were added in the multiple regression analyses, and tested for significance. Model II shows that learning (the one-factor solution) moderates the relationship between SOC and its predictor, task significance (standardized β for the interaction term is .11, p=0.012), corrected for the effects of social relations, job control, and age. In turn, Model III shows that learning moderates the relationship between task significance and its predictor, SOC (standardized β=0.13, p=0.005). When its sub-constructs are examined, the regression analysis in model IV shows that instrumental learning moderates the relationship between job control and its predictor, SOC (standardized β=0.14, p=0.002). So, out of the 24 possible moderating effects, only three were found to be significant, thereby giving only a weak confirmation of hypothesis 2.
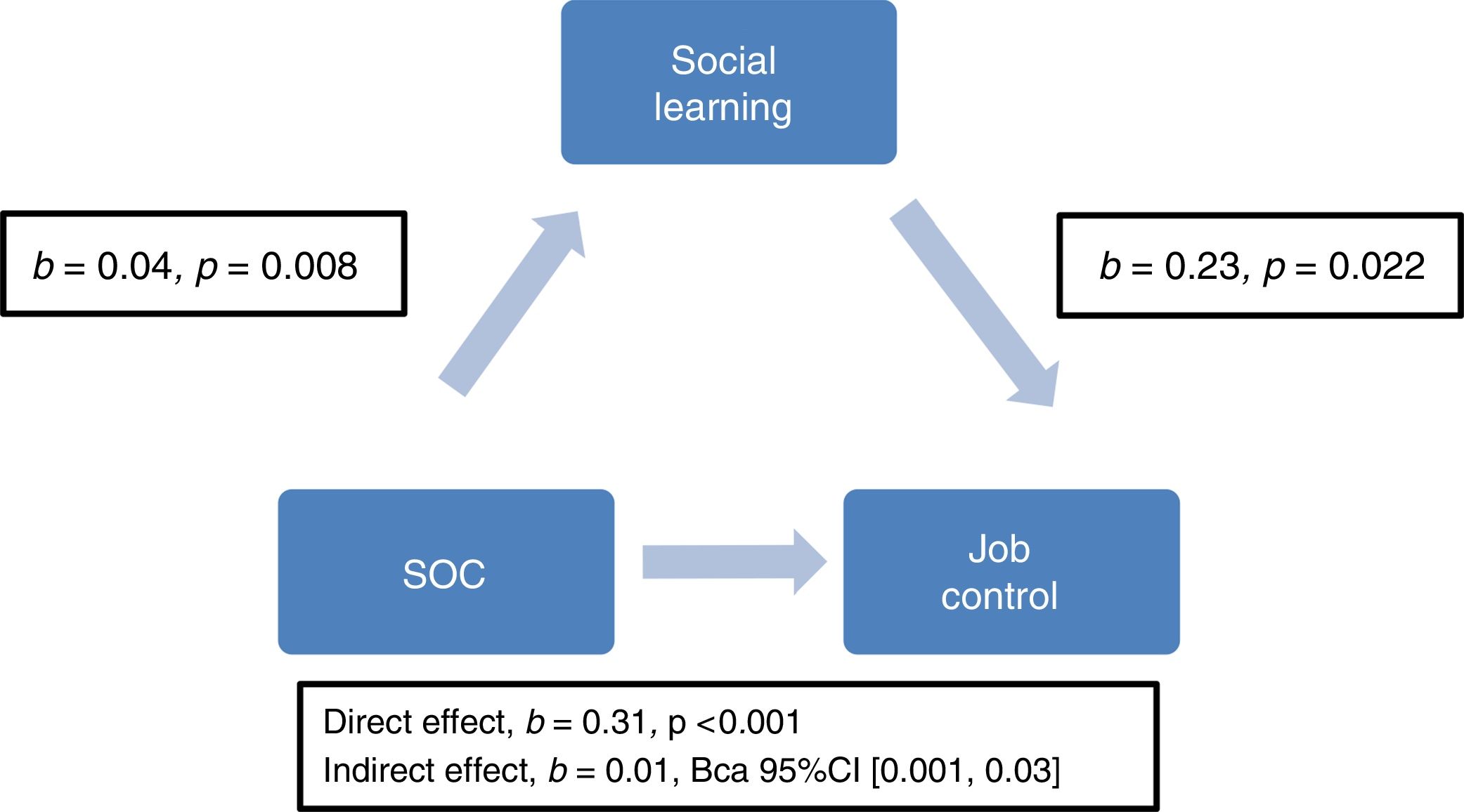
Mediating effectsSimple mediation analyses –examining each mediator variable separately– showed that social learning mediates the relationship between job control and its predictor, SOC, b=0.01, BCa 95%CI [0.001-0.03] corrected for the effects of age. This supports hypothesis 3 (Fig. 1). However, no other indirect effects of learning were found within the relationship between SOC and GRRs.
DiscussionReciprocal relationship between SOC and the three GRRs
As hypothesized, the present findings show that social relations, task significance, and job control explain variance in SOC. Moreover, each of the three GRRs contributes very significantly after correcting for the effects of the other two GRRs and age. This suggests that the stronger SOC is, the stronger the scores on these three GRRs, and vice versa. The findings align with Antonovsky's9,38 suggestion that a resourceful work environment strengthens employees’ view of the world as comprehensible, manageable, and meaningful.
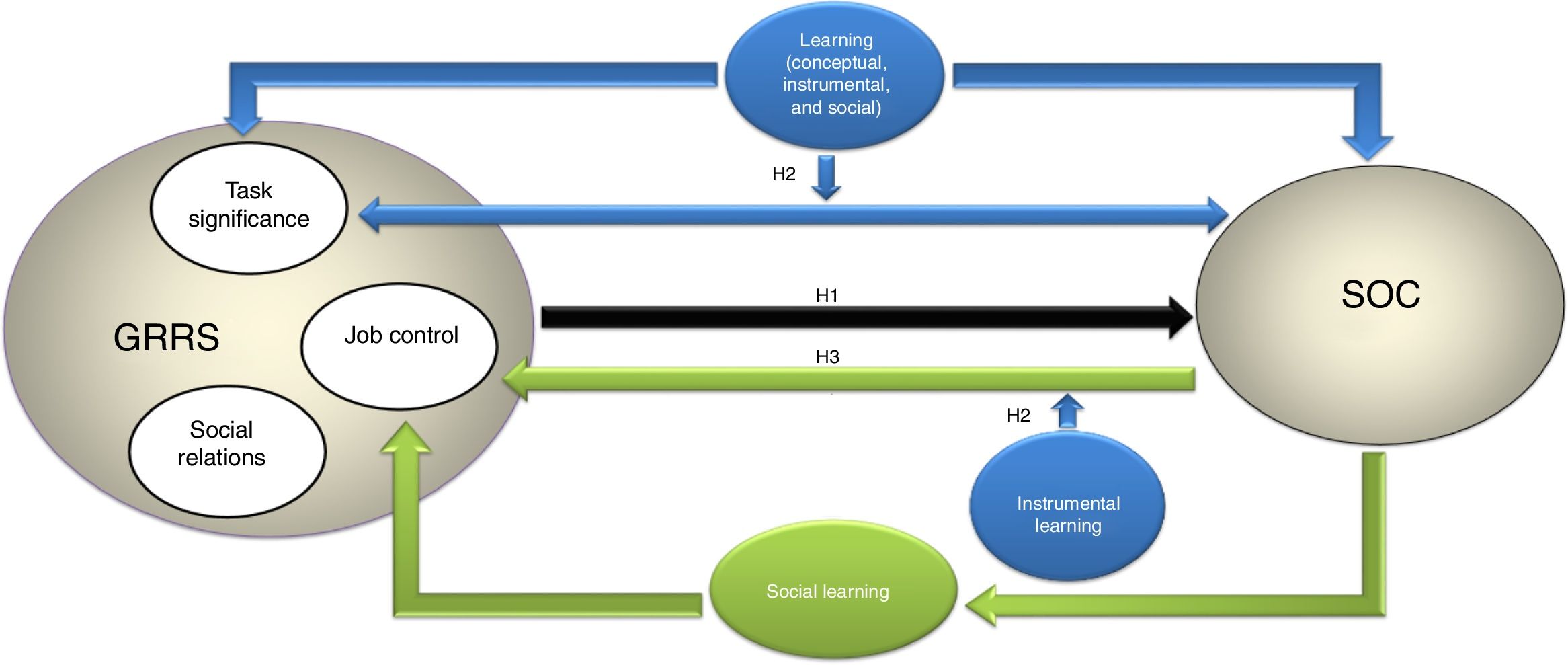
Moderating and mediating effects of learningThe results of the analysis in the context of the model used are summarized in Figure 2. The findings indicate that the overarching learning concept moderates the relationship between SOC and task significance corrected for the effects of social relations, job control, and age. This interaction effect suggests that, when learning is higher, the relationship between SOC and task significance is stronger; this is in line with salutogenic theory. Learning can enhance the perception of employees that their job has a positive impact on other people, which is important for the development of their SOC.6

The present study shows that instrumental learning moderates the relationship between job control and SOC. This interaction effect indicates that a strong SOC together with the development of skills through courses or learning on the job builds an employee's job control. Social learning mediates this relationship, which suggests that a strong SOC fosters learning through cooperation, feedback, sharing experiences, but also through job challenges like the growth of responsibilities or changes in tasks and functions, all of which also builds an employee's job control. Social relations were not involved in any of the moderating and mediating effects. It should be noted that the moderating and mediating effects of learning were relatively small. Also, conceptual learning on its own did not show any moderating or mediating effects, whereas instrumental and social learning on their own did. This suggests that other factors could play a role in the relationship between SOC and GRRs in workplaces.
The results of this study can be used to develop health and wellbeing of nurses and caregivers to a certain extent. Maintaining and developing health and wellbeing of healthcare workers is essential since the quality of care provided strongly depends on their health and wellbeing.4 To enhance instrumental and social learning in healthcare organizations, a central role should be given to healthcare workers themselves because they know the best what is needed to find a good fit with the work environment.6 Achieving this fit enables them to not only learn through formal activities, but also through cooperation, feedback, sharing experiences, and job challenges, which could strengthen their SOC and build their GRRs.
Although the average age of the total sample was lower than the study population, the percentage of male and female healthcare workers in this particular sector reflects the study population.29 Also, SOC did not significantly differ between them, which indicates that the findings of this study may be generalized to both males and females. However, due to the feminization of the nursing profession,39 learning processes may differ among men compared to their female counterpart. Also, age should be taken into account since the relevance of the GRRs and learning may differ between nurses and caregivers at different ages.
Study limitationsThe present study has some limitations that should be taken into account. First, as all measures were self-reported, common method biases may have influenced the results.40 However, constructs such as SOC are difficult to measure using methods other than self-reporting.2,31
A second concern is the cross-sectional study design used to test for mediating effects. Longitudinal designs are required to provide evidence for the mediating roles of variables.41 Since this study indicated that social learning mediates the relationship between job control and SOC, future studies may aim to validate this finding using a longitudinal design.
A third issue is that the original dataset (N=758) was reduced to only those respondents who had completely answered all the SOC and the WLPQ items (N=481). However, the differences presented in Table 1 did not deviate from the differences in the original dataset. Moreover, by excluding the incomplete responses regarding these items, the exploratory factor analysis and reliability analysis were enhanced.42
Another concern is that the response rates were lower than the expected 38%. However, this study reconfirmed the difficulty of achieving a high response rate among healthcare workers.30 Future studies are recommended to already involve nurses and caregivers in the design phase of the survey,43 use a mail survey mode combined with monetary incentives,30 or promise that the outcomes will be used to enhance workplace health promotion policies, which can result in higher response rates compared to an online questionnaire without financial compensation.30
A final point worthwhile discussing is that the Facebook group also included nurses and caregivers from other healthcare settings, such as hospitals. However, the aim of this study was not to test for invariances across specified subgroups. Nevertheless, future studies may aim to validate the findings of this study across specified subgroups, for instance, among healthcare workers in hospitals.
ConclusionsThis study shows that a resourceful work environment strengthens the ability of healthcare workers to develop health and wellbeing, which is essential because the quality of care provided depends on their health and wellbeing. Conceptual, instrumental, and social learning, combined, enhances employees’ perception that their work has a positive impact on other people, which strengthens their SOC. Healthcare workers develop skills through courses or learning on the job, but also through cooperation, feedback sharing experiences, and job challenges. Form a health promotion perspective, it is therefore worthwhile to invest in instrumental and social learning of healthcare workers.
Editor in chargeCarlos Álvarez-Dardet.
Transparency declarationThe corresponding author on behalf of the other authors guarantee the accuracy, transparency and honesty of the data and information contained in the study, that no relevant information has been omitted and that all discrepancies between authors have been adequately resolved and described.
Research suggests that a resourceful work environment contributes to employees’ ability to view the world (work) as comprehensible, manageable, and meaningful. A strong sense of coherence has a health-promoting effect, and building generalized resistance resources has a more sustainable effect than reducing job demands.
What does this study add to the literature?There is a relationship between sense of coherence and the generalized resistance resources (social relations, task significance, and job control), which seems to be strengthened or explained by instrumental and social learning to a certain extent. A salutogenic workplace could be built by fostering instrumental and social learning, which requires a good fit between employees and their work environment through keen employee participation.
R. Pijpker, L. Vaandrager and M. Koelen conceived the study. R. Pijpker coordinated and conducted the field work. R. Pijpker and L. Vaandrager piloted the questionnaire. R. Pijpker and EJ. Bakker executed the statistical analysis. All authors read and commented on the final version of this manuscript.
FundingNone.
Conflicts of interestNone.
The authors are grateful to the employers and employees of the four healthcare organizations that participated in this study: Noord Nederlandse Coöperatie van Zorgorganisaties (NNCZ); Woon- en zorgcentrum de Westerkim; Zorgcollectief Zuidwest-Drenthe; and Woonzorgcentrum ‘t Derkshoes. We also thank N. Jacobs-Seegers for giving permission to place the self-administered questionnaire on the healthcare-related Facebook group. Special thanks to Gaby Ortiz Barreda (University of Bergen, Norway) and Anna Bonmatí Tomàs (University of Girona, Spain) for translating the abstract into Spanish. Finally, we appreciated Catherine O’Dea's contribution to the manuscript.
Supplementary data associated with this article can be found, in the online version, at https://www.youtube.com/edit?o=U&video_id=YYdHNqp07P8.











