




To qualitatively analyze the abuse situations, as well as victims’ perception on the resources needed for reporting and prevention.
MethodInterviews with 10 medical students and 15 medical residents were conducted using a semi-structured questionnaire. The interviews were interrupted once saturation was reached in both aspects of the research subject. Information was collected using pre-designed outlines and completed with transcribed notes at the end of each interview.
ResultsA range of power abuse behaviors were identified, including social exclusion, hierarchical dynamics, and insufficient teaching and mentorship. Participants reported arbitrary favoritism of colleagues in the allocation of on-call duties. Instances of mockery, verbal abuse, and racial slurs were described. Gender-based discrimination manifested through sexist remarks and the sexualization of female physicians, including inappropriate comments and unsolicited advances, such as non-consensual touching and kissing. Victims frequently refrained from reporting these events due to fear of retaliation or a lack of awareness regarding available reporting mechanisms. Participants emphasized the need for preventive and protective strategies, and proposed training in labor rights and medical professionalism, alongside mentorship by educators genuinely committed to teaching, as essential preventive measures.
ConclusionsThe results of this initial investigation support the notion that abuse is part of the medical training process. Victims identified multiple preventive strategies that merit consideration at the institutional level within both academic and healthcare settings.
Analizar cualitativamente las situaciones de abuso padecido, así como la percepción sobre los recursos necesarios para su denuncia y prevención.
MétodoSe realizó una entrevista semiestructurada a 10 estudiantes de medicina y 15 médicos residentes. Estas se interrumpieron al alcanzar la saturación de respuestas. La información fue recopilada utilizando un esquema prediseñado y completado con notas transcritas.
ResultadosSe identificó una variedad de formas de abuso, incluyendo exclusión social, dinámicas jerárquicas y enseñanza y supervisión insuficientes. Los y las participantes informaron de favoritismos arbitrarios en la asignación de guardias. Se describieron casos de burlas, abuso verbal e insultos raciales. La discriminación de género se manifestó mediante comentarios sexistas y la sexualización de médicas, incluyendo comentarios inapropiados y conductas no consentidas, como tocamientos y besos. Las víctimas frecuentemente se abstuvieron de denunciar estos hechos por miedo a represalias o desconocimiento de los mecanismos disponibles para hacerlo. Los y las participantes enfatizaron la necesidad de estrategias preventivas, y propusieron la formación en derechos laborales y profesionalidad médica, junto con la tutoría por parte de docentes vocacionales, como medidas preventivas.
ConclusionesLos resultados de esta investigación inicial apoyan la idea de que el abuso forma parte de la educación médica. Las víctimas identificaron múltiples estrategias preventivas que requieren la participación institucional de los sistemas académicos y sanitarios.
Abuse of medical students and medical residents within medical practice has been documented since 1982, when HK Silver likened this phenomenon to child abuse.1 These detrimental behaviors, perpetrated by healthcare professionals, non-health professionals, patients and families have been corroborated by numerous international studies.2–7 Beyond the immediate harm to victims’ health and well-being, such behaviors contribute to adverse outcomes, including elevated rates of burnout among mistreated medical students and medical residents,6,8 and a demonstrable decrease in the quality of patient care and professional commitment.9
Studies investigating sexual harassment of medical residents and attending physicians —primarily through surveys—, show a high prevalence of verbal, non-verbal, physical abuse or sexual harassment in the clinical environment.10–13 Furthermore, significant knowledge gap exists regarding appropriate response to these incidents.10 Notably, a study of General Surgery Residents in Spain reported psychological abuse in 73.9% of respondents, gender discrimination in 55.1%, physical mistreatment in 7.1%, and burnout symptoms in up to 47.6% of residents, with 4.6% reporting suicidal ideation.14
Intervention strategies for abuse prevention, including educational programs or fostering a zero-tolerance culture, have already been proposed, with some demonstrating promising experimental results.15,16
Despite the severe repercussions of abuse in medical training, research exploring the victim's perspective, encompassing the characteristics and typologies of abuse, as well as perceptions on potential preventive interventions, remains limited.
This research aims to achieve two primary objectives: first, to conduct a qualitative analysis of abuse situations experienced by medical students and medical residents; and second, to investigate their perceptions regarding the resources and actions necessary for reporting and prevention.
MethodApproach and study designA qualitative approach with semi-structured interviews was used to explore experiences and perceptions of abuse and its prevention or report.
Questionnaire design and pilot phaseA semi-structured questionnaire was developed through a series of team meetings and iterative revisions until a consensus was reached on the initial version. The preliminary draft comprised four sections: demographic data, experiences of abuse, preventive measures and an open-ended section for additional comments.
The interview format and procedures underwent a pilot phase involving two medical students and two medical residents to evaluate feasibility and clarity, and to identify areas for improvement. This phase also facilitated an assessment of the instrument's reliability. Particular attention was given to the practicality of online administration, the adequacy of interviewer notes as a data collection method, respondent comfort, and the wording of the questions. Feedback obtained during this stage culminated in the final version of the interview guide (see online Supplementary data).
Sample and selection of participantsParticipants were selected using a snowball sampling method based on contacts from the researchers. The first participants were contacted personally trough social media or email in March 2024, date in which the field work began. After that, every participant shared the project with colleagues, who directly contacted the investigation team until September 2024, when the data collection finished. The sample included a total of 10 medical students (4 men and 6 women) and 15 medical residents (7 men and 8 women), all of them studying or working in public institutions. The mean age was 23 (22-26) for the students and 28 (25-33) for the residents. All the medical students were in the 5th or 6th year of the degree. There were at least 3 medical residents for each of the first four residence years. Every student and resident contacted agreed to participate, turning out in 0 rejections. There were no withdrawals.
The study was approved by the Ethics Committee of Miguel Hernández University. Informed consent was obtained from all participants prior to their involvement in the study.
Data collection and analysisBefore the interview, participants were granted with a document with a brief introduction of the reason and objectives of the study and the information gathering methods. In order to ensure participants anonymity and allow a more comfortable situation to share information, any audio nor video of the meetings was recorded. Instead, data were captured in real-time through interviewer notes using a predefined template, complemented by a written report completed immediately after each interview. To avoid potential biases, the fulfilled templates were not handed to the participants and there was not opportunity to repeat the interviews.
During the meetings there were just two people, the participant and the first author. All interviews were online via video call whit an average duration from 45 to 90minutes.
An inductive thematic analysis was conducted. We focused on the content of what was said and we identified, examined, and reported patterns or themes that emerged directly from the data itself, without imposing categories or preconceived theoretical frameworks from the research team. Initial coding was performed by one researcher and subsequently reviewed and discussed with a second researcher. Discrepancies were resolved through internal team consensus. A total of 26 codes were agreed upon which were later grouped into 3 categories, corresponding to the headings presented in the Results section. No qualitative data analysis software was used; coding was conducted manually.
Data saturation began to emerge after the 15th interview; however, data collection continued to ensure maximum sensitivity in detecting both the types of abuse and the preventive interventions perceived as necessary, resulting in a total of 25 interviews.
ResultsAbuse was defined as all those avoidable, unnecessary, and harmful attitudes by health and non-health professionals, patients and family members that have a negative impact on the victim's learning, health and quality of life.
Some examples of textual quotations can be found at the end of the section (Table 1). An additional file contains tables with all textual quotations obtained from the interviews that complement the results reading (see Tables 1-3 in online Supplementary data) and another one with the same content in the original language of the interviews (see Tables 1-3 in online Supplementary data).
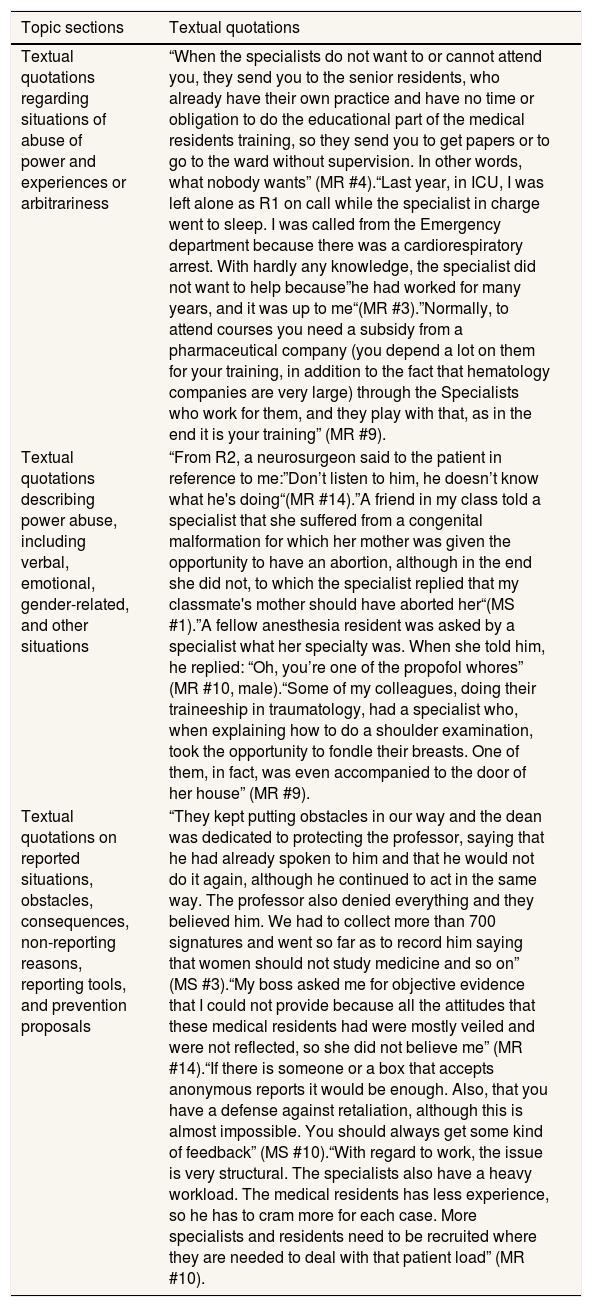
Examples of textual quotations.
| Topic sections | Textual quotations |
|---|---|
| Textual quotations regarding situations of abuse of power and experiences or arbitrariness | “When the specialists do not want to or cannot attend you, they send you to the senior residents, who already have their own practice and have no time or obligation to do the educational part of the medical residents training, so they send you to get papers or to go to the ward without supervision. In other words, what nobody wants” (MR #4).“Last year, in ICU, I was left alone as R1 on call while the specialist in charge went to sleep. I was called from the Emergency department because there was a cardiorespiratory arrest. With hardly any knowledge, the specialist did not want to help because”he had worked for many years, and it was up to me“(MR #3).”Normally, to attend courses you need a subsidy from a pharmaceutical company (you depend a lot on them for your training, in addition to the fact that hematology companies are very large) through the Specialists who work for them, and they play with that, as in the end it is your training” (MR #9). |
| Textual quotations describing power abuse, including verbal, emotional, gender-related, and other situations | “From R2, a neurosurgeon said to the patient in reference to me:”Don’t listen to him, he doesn’t know what he's doing“(MR #14).”A friend in my class told a specialist that she suffered from a congenital malformation for which her mother was given the opportunity to have an abortion, although in the end she did not, to which the specialist replied that my classmate's mother should have aborted her“(MS #1).”A fellow anesthesia resident was asked by a specialist what her specialty was. When she told him, he replied: “Oh, you’re one of the propofol whores” (MR #10, male).“Some of my colleagues, doing their traineeship in traumatology, had a specialist who, when explaining how to do a shoulder examination, took the opportunity to fondle their breasts. One of them, in fact, was even accompanied to the door of her house” (MR #9). |
| Textual quotations on reported situations, obstacles, consequences, non-reporting reasons, reporting tools, and prevention proposals | “They kept putting obstacles in our way and the dean was dedicated to protecting the professor, saying that he had already spoken to him and that he would not do it again, although he continued to act in the same way. The professor also denied everything and they believed him. We had to collect more than 700 signatures and went so far as to record him saying that women should not study medicine and so on” (MS #3).“My boss asked me for objective evidence that I could not provide because all the attitudes that these medical residents had were mostly veiled and were not reflected, so she did not believe me” (MR #14).“If there is someone or a box that accepts anonymous reports it would be enough. Also, that you have a defense against retaliation, although this is almost impossible. You should always get some kind of feedback” (MS #10).“With regard to work, the issue is very structural. The specialists also have a heavy workload. The medical residents has less experience, so he has to cram more for each case. More specialists and residents need to be recruited where they are needed to deal with that patient load” (MR #10). |
ME: medical student; MS: medical resident.
In response to the general inquiry regarding experiences of power abuse, almost all the interviewees reported feeling invisible or systematically ignored, primarily by the attending specialists within the departments where they were assigned. These experiences were also attributed to residents and, less frequently to nursing staff.
More than half of the interviewees expressed, either explicitly or implicitly, a perception that physicians were disinterested in supervising or engaging with students. Additional concerns were raised regarding early dismissal from clinical duties, a lack of structure and information related to clinical placements, and, in descending order of frequency, instances of discourteous or disrespectful behavior from healthcare professionals.
Regarding medical residents, the most frequently cited issue was the highly hierarchical nature of departmental environments, which appeared to foster systemic mistreatment of individuals in subordinate positions.
Other recurring concerns included inadequate supervision during the first year of residency (particularly in emergency departments), insufficient educational support, excessive workloads that were disproportionate to the residents’ level of training, non-compliance with official working hours, hostile communication from supervisors, and a negative work environment.
In the university context, fewer instances were reported. However, students highlighted recurring inappropriate remarks from certain lecturers, non-compliance with university regulations or the official teaching syllabus, and instances of mocking behaviour.
Slightly more than half of the students reported experiences of arbitrary treatment. These included perceived favoritism towards certain students, exclusion from operating theatres without standardized criteria, and the assignment of clinical tasks or internships based on personal relationships rather than merit.
Residents reported a higher number of arbitrary practices, particularly regarding on-call scheduling. It was noted that the allocation of on-call shifts was often influenced by personal relationships with fellow residents or attending physicians, serving either as a form of reward or punishment with direct implications for financial compensation. One-third of the residents also identified preferential treatment of certain colleagues, while a smaller proportion reported conditional access to procedural training based on their rapport with supervising specialists, sometimes involving coercive or manipulative dynamics.
Emotional, racist, gender-based, sexual and other forms of abuseVerbal or emotional abuse directed toward medical students was frequently reported, particularly in the form of mockery by the supervising specialists. Students described being subjected to teasing and taunting, often related to their perceived lack of knowledge. Several testimonies included instances in which professionals posed compromising or inappropriate questions concerning political opinions or personal information about colleagues within the department.
Most of the residents reported having experienced public verbal abuse, mockery and humiliation being insulted, taunted and ridiculed in public, primarily at the hands of adjuncts physicians, senior residents or professionals from other specialties. In some cases, such behaviours were attributed to patients, especially within emergency departments and operating theatres. Residents further reported being accused of lacking clinical competence or skills.
One of the interviews revealed particularly serious incidents, including shouting, expressions of anger, use of derogatory nicknames, psychological manipulation, and even a case of physical assault by a specialist directed at a resident.
Incidents of racially motivated abuse were less frequently reported by students and typically involved isolated episodes of verbal insults, inappropriate comments, or deliberate exclusion. Among residents, there were a few reports of perceived discrimination against racialized individuals, occasional verbal aggression from patients or specialists, and racist remarks.
Regarding gender-based discrimination among students, many reported situations in which their knowledge or clinical ability was implicitly or explicitly questioned. Reports also included disrespectful treatment toward female students, experiences of sexist comments, personal inquiries about partners, misidentification as nursing staff, and the preferential selection of male students for technical procedures or clinical examinations.
Residents highlighted inappropriate behaviour from patients, including diminished respect for female physicians, refusal to be treated by women despite prior introductions, and repeated confusion between female doctors and nurses. Reports also pointed to sexist remarks by specialists -predominantly male-, including the sexualization of female doctors, preferential allocation of technical procedures to male residents, overall better treatment of men, questioning the competence of female residents, and holding them to higher performance standards.
Regarding sexual harassment, some students reported having received inappropriate sexual comments, suggestive insinuations, and occasional boundary-crossing behaviour. Residents disclosed being subjected to lewd remarks, unsolicited sexual questions, and instances of inappropriate physical contact, including unwanted touching or kissing without consent.
Nearly half of the residents and one student reported exposure to homophobic or transphobic insults or comments, as well as unpleasant behaviour targeting individuals with overweight or disabilities.
Prevention and control interventionsAbuses reported by medical students and residents led to formal complaints in 4 medical students and 6 medical residents. The students used teaching quality surveys, the collection of signatures, contact with university entities or public reports. They reported obstacles in the process, mainly from the university or colleagues defending the accused individuals. In contrast, independent university institutions, such as gender and identity observatory, initiated internal investigations more easily. The residents generally reported incidents internally or through hospital committees. Difficulties were reported due to the lack of a clear reference person to report problems involving their tutors. Sometimes the issue was minimized or the person making the report was not believed because he or she was unable to provide evidence of situations that were being concealed.
In some cases, the resolution process was not known or no response was received. In others, interviewees expressed satisfaction with actions such as eliminating a rotation or forcing teachers to take a course. Nonetheless, some participants reported that no action or unsatisfactory action was taken. One person reported a deterioration in their relationship with supervisors.
Students often choose not to report abusive situations for a variety of reasons, most notably being fear of reprisals and lack of knowledge about the tools to use. According to the residents, the two main barriers identified for not reporting were fear of reprisals and the assumption that the report would not be useful.
The normalization of abuse is also widespread. Some respondents prefer not to create a hostile working environment, do not feel able to prove situations or perceive a lack of confidentiality.
Most respondents expressed the need for a mechanism through which to report. Students mainly mentioned the availability of anonymous boxes and surveys. The residents, on the other hand, emphasized the importance of having a reference person to guide them through the reporting process- someone external to their department, hospital, or even outside the trade union structure.
Additional suggestions included the creation of a support group among themselves and assistance in defending against possible reprisals, the development of reporting protocols, disrupting the power relationship and avoiding the normalization of abuse.
Many interviewees emphasized the importance of training in labor rights, medical professionalism and mentoring of students and residents by those professionals who are committed to teaching or, only those who are also teachers should be mentors. Anonymous and public quality surveys were also proposed as a preventive tool, with the recommendation that their results be used to influence the assessment of both hospitals and academic institutions.
The possibility of legislating teaching practice was also considered, introducing rules that reward correct behavior and punish abuse. Some suggested that a portion of the salary of those specialists working in university hospitals should depend on the evaluation of the students.
Several interviewees stressed the need to empower both victims and colleagues to increase the number of reports.
Measures aimed at structural work also stand out, such as encouraging mentorship by younger professionals, breaking the hierarchical chain of abuse, reducing the workload (including 24-hour days on call) and avoiding the delegation of teaching responsibilities for medical students to residents.
Some residents have also suggested the use of specific assessment criteria to reduce subjectivity.
When asked which group was most appropriate to work with, the majority of respondents considered the importance of addressing the adjuncts and chiefs of department, while another group highlighted the need to address residents and medical students as future professionals.
DiscussionThis qualitative study addresses the dynamics of abuse in the medical sphere, offering insight into its manifestations and consequences. All medical students and medical residents reported having experienced abusive situations during their training. Most chose not to report these events. Moreover, this finding highlights an urgent need for preventive strategies to curb power abuses within the academic and clinical environments of medical education. As stated in a Lancet editorial,17 the normalization of inappropriate behaviors within medical training is evident, generating conflicts with medical ethics and the core values of professionalism, including collaborative practice, support for learning, and the fostering of constructive critical inquiry.
The qualitative approach allows us to understand first-hand the experiences and contexts in which abuse has occurred and the perceptions of those who have experienced it, including their suggestions for improving the current situation. Direct contact with the interviewees allowed for a wide variety of responses and yielded a rich volume of data.18 The participants considered the study to be relevant and provided as much information as possible. Perceptions reported by the vast majority of respondents have been identified, lending strength to the findings.
In terms of weaknesses, the sample size may seem small, however, as this is a qualitative study, sampling was guided by response saturation.19 Regarding sample diversity, interviews were conducted with participants from various universities and hospitals. With regard to the specialty of the residents, most were from Family and Community Medicine. However, experiences from acquaintances in other specialties were also reported, allowing for broader thematic coverage. The interviewees volunteered, which may introduce participation bias, but the aim of this study is explanatory rather than quantitative, thus the goal is not to generalize findings, but rather to deepen understanding of the phenomenon. Although certain quotes may appear limited when viewed in isolation, they should be interpreted within their broader critical and thematic context. What has been gathered are individual perceptions of what each participant identifies as abusive behavior. The fact that the interviewer was also a medicine student could lead to misunderstandings in the gathering of information due to similar experiences to the narrated ones. In that sense, when a comment was not clear, it was demanded to be explained with more details. The interview guide was a useful tool to minimize the investigator bias.
To the best of our knowledge, this is the first qualitative research study specifically addressing this issue, so it cannot be compared with similar studies. The most similar published articles are quantitative in nature, using individual surveys which focus primarily on gender discrimination and abuse in medical residents-often excluding the university population and perceptions of necessary interventions.5–14 While these quantitative studies are valuable for measuring the magnitude of the issue, they do not explain its underlying dynamics. This is why this work complements existing data, by offering deeper insights into the causes, distribution and perceived measures for addressing abuse in medical training.
Similarly, qualitative data would need to be gathered on the impact on the quality of life and health of the victims of abuse and those who depend on them, since existing studies are predominantly quantitative in nature.2–4,7,9
The results obtained reveal structural issues in the training of doctors in Spain. This is further supported by findings from an anonymous survey conducted among women working in healthcare services and academia in Spain.15 Up to 73.6% of respondents said they had experienced sexual harassment, and 28.7% said they had experienced sexual abuse. Consistent with our results, participants were reluctant to report these incidents, in part due to the near-complete lack of consequences for perpetrators. This study has also observed what our results describe in the sense that there is a growing awareness among victims, who are beginning to demand concrete action. This necessitates the active involvement of public administrations, healthcare systems, and universities to understand the situation and implement appropriate measures. Inaction is not an option, and although context-specific research on the effectiveness of interventions is needed, there is already a sufficient body of described interventions that can be implemented.16 Participatory approaches, in particular, have been reported to yield the most promising outcomes.
The findings of this research align with the notion that abuse of power is a constant throughout the medical education process at different levels. Furthermore, they highlight the need to design and implement prevention and reporting plans. Therefore, further research is necessary to explore the various dimensions of abuse and to evaluate the effectiveness of the intervention proposals.
Availability of databases and material for replicationThe pre-designed outline can be demanded from the corresponding author. Database is not available due to privacy and personal and confidential information provided by victims of abuse.
There is information provided by quantitative studies that shows high levels of sexual discrimination in the medical environment, including training, and different abuse forms through medical residents, which is linked to burn out, low quality of patience care and suicidal ideation. Little intervention projects have been tested to solve this issue.
What does this study add to the literature?This may be the first qualitative study in the field, where the victims describe how the abuse is committed and perpetuated and their perception of solutions and prevention. It also grants the point of view of university students.
What are the implications of the results?Our results may guide the health training policies to obtain a healthier and more effective learning process and may be the basis for new intervention projects where the proposed solutions by the victims themselves were tested.
Alberto Lana.
Transparency declarationThe corresponding author, on behalf of the other authors guarantee the accuracy, transparency and honesty of the data and information contained in the study, that no relevant information has been omitted and that all discrepancies between authors have been adequately resolved and described.
Authorship contributionsC. Sánchez-Miralles contributed to the conception of the study, design of the questionnaire, interview of the participants, data analysis, interpretation of results and editing of the manuscript. C. Blanes-Mira contributed to the design of questionnaire, data analysis, interpretation of results and editing of the manuscript. I. Hernández-Aguado contributed to the conception of the study, data analysis, interpretation of results and editing of the manuscript.
AcknowledgmentsTo Elisa Chilet-Rosell for reviewing the manuscript and for her suggestions.
FundingNone.
Conflicts of interestsNone.














