



Road traffic accidents cause substantial morbidity and disease burden; few studies have examined their impact on disability.
ObjectiveTo estimate the magnitude and distribution of disability due to road traffic accidents according to socio-demographic variables, and its main socioeconomic and health determinants.
MethodsA cross-sectional study was conducted in community-dwelling participants in the “2008 Spanish National Disability Survey”, a representative sample of 91,846 households with 20,425 disabled persons older than 15 years; 443 had disability due to road traffic accidents.
ResultsThe prevalence was 2.1 per 1000 inhabitants (95% CI:1.8-2.3), with no differences by sex. Risk was highest among persons aged 31 to 64 years, and onset of disability showed a sharp inflection point at age 16 years in both sexes. Odds ratios (ORs) were higher (OR=1.3; 95% CI:1.1- 1.7) for participants with secondary education than for those with the lowest educational levels and were lower (OR: 0.5; 95% CI:0.3-0.8) for participants with the highest household income levels than for those with lowest. Only 24% of disabled participants were gainfully employed. As compared to other sources of disability, traffic crashes caused greater disability in terms of mobility (OR=3.1;p<0.001), a greater need for health/social services (OR=1.5;p=0.003), and more problems with private transportation (OR=1.6;p<0.001), moving around outside the home (OR=1.6;p<0.001) and changes in economic activity (OR=2.4;p<0.001).
ConclusionsThe prevalence of disability due to road traffic accidents in Spain is lower than in other developed countries, with middle-aged and socio-economically underprivileged persons being the most affected. Disability due to road traffic accidents is related to a greater demand for social/health care support, problems of accessibility/commuting, and major changes in economic activity.
Los accidentes de tráfico causan importante morbilidad y carga de enfermedad; su impacto sobre la discapacidad ha sido poco estudiado.
ObjetivoEstimar la magnitud y distribución de la discapacidad por accidentes de tráfico según variables socio-demográficas, y sus principales condicionantes socio-sanitarios y económicos.
MétodosEstudio transversal en participantes de la Encuesta Nacional de Discapacidad, Autonomía Personal y Situaciones de Dependencia 2008; muestra representativa de 91.846 hogares con 20,425 discapacitados mayores de 15 años, 443 causados por accidentes de tráfico.
ResultadosLa prevalencia fue de 2,1 por 1000 (IC 95%: 1,8-2,3), sin diferencias por sexo y mayor riesgo entre 31-64 años. La discapacidad tuvo inicio abrupto a los 16 años (ambos sexos). Aquellos con educación secundaria tuvieron un mayor odds ratio OR (OR=1,3; IC 95%: 1,1- 1,7) que aquellos con menor nivel educativo; los discapacitados con mayores ingresos tuvieron menor OR (OR=0,5; IC 95%: 0,3-0,8) que aquellos con ingresos más bajos. Sólo un 24% tenían empleo remunerado. Comparado con otras causas de discapacidad, los accidente de tráfico generaron mayor discapacidad en movilidad (OR=3,1;p<0,001) y necesidad de asistencia socio-sanitaria (OR=1,5;p=0,003); mayores problemas con el transporte privado (OR=1,6;p<0,001), los desplazamientos fuera de casa (OR=1,6;p<0,001) y cambios en la actividad económica (OR=2,4;p<0,001).
ConclusionesLa prevalencia en España es baja comparada con otros países desarrollados. La población de mediana edad y con desventajas socio-económicas fue la más afectada. La discapacidad por tráfico se relaciona con mayor demanda de servicios socio-sanitarios, problemas de accesibilidad y movilidad e importantes cambios en la actividad económica.
Injuries caused by road traffic crashes (RTCs) have a major impact on morbidity, mortality and premature disability. According to the World Health Organisation (WHO), every year there are over 1.2 million deaths due to this cause around the world, 20 to 50 million persons sustain injuries, and more than 5 million remain disabled for life.1 RTCs cause disability in the short and long term, are the 9th leading cause in the world of disability-adjusted life years (DALYs) and generate 41.2 million years of healthy life lost, thus accounting for 2.7% of the total worldwide.2–5It is estimated that there are 3.8 million disabled persons in Spain. Accidents are the 3rd leading cause of disability and account for 9% of all disability; within this category, RTCs rank second after occupational accidents.6
Despite the appreciable reduction in traffic accident figures observed in this country from 2000 onwards,7 the resulting injuries continue generating a substantial disease burden, with a great impact on the country's social and economic spheres. RTCs generate premature mortality,8 continue to be the leading specific cause of death in the 15-34 year age group, and are the leading (in men) and 2nd leading cause (in women) of years of potential life lost.9
On investigating the effects on RTC-injury victims, analysis of disability can provide a complementary view of this event and furnish the necessary information for the prevention and control of RTCs, and so minimise the risk of premature death, disability and sequelae. Road traffic disability (RTD) is an important indicator of the severity of such accidents, and allows for assessment of related temporary or permanent disability, loss of autonomy, individual development disorders, family involvement and the ensuing social burden.10
The aim of this study was thus to provide a first-ever estimate of the magnitude and distribution of disability caused by RTCs in Spain, and to describe the RTC-disabled population by reference to basic socio-demographic variables, as well as the types of RTC-related disability and their main socio-economic and health profiles.
MethodsStudy design and populationA cross-sectional study was conducted among community-dwelling participants of the “2008 National survey of disability, personal autonomy and situations of dependency” (EDAD2008). The survey covered all regions of Spain from November 2007 to February 2008, targeting all persons residing in main family dwellings.11
The EDAD2008 was based on a two-stage, stratified sampling design, with the first-stage units being census sections and the second-stage units being main family dwellings. A sample size of 96,075 households was established. Response was obtained from 91,846 households (overall response rate of 97%),12 yielding data on 213 626 subjects, including 20,425 disabled persons over the age of 15 years, 443 of whom had disability due to traffic crashes. The data-collection method used was the personal interview.11
Study variablesThe EDAD2008 partly follows the conceptual framework of the International Classification of Functioning, Disability and Health (ICF),13 according to which disability is defined as, “a set of limitations on activities of daily living and participation restrictions (handicaps), which have lasted or are envisaged to last for more than one year and have their origin in some impairment, even though they may have been overcome with the use of external technical aids or with the aid or supervision of another person.“For study purposes, RTD was defined as, “any type disability caused by a road traffic accident”, and analysed using the following independent variables: sex; age (four groups); educational level (no formal education/primary; secondary/intermediate; higher/university); marital status (single; married; widowed; divorced/separated); nationality (Spanish; foreign/dual); occupation (employed; unemployed; receiving any type of pension; unfit for work; other non-remunerated activity); net monthly household income (<€500; €500-<€1,500; €1,500-<€3,000; >=€3,000); type of disability (vision; hearing; communication; learning, application of knowledge and performance of tasks; mobility; self-care; domestic life; interpersonal interactions/relationships); age at disability onset (exact age); health and social conditions (health status; need of consultation/health/social services; type of help received; financial benefit or compensation; problems with transport and commuting); economic conditions (primary household earner; change in economic activity; reason for leaving work; expenditure in the preceding year; and main items of expenditure).
Statistical analysisWe calculated the crude prevalence and its 95% confidence interval (CI), using the total number of persons surveyed over the age of 15 years (n=213 626) as the reference population. The distribution according to socio-demographic variables was summarised with odds ratios (ORs) obtained from logistic regression models, controlling for all socio-demographic variables simultaneously. We calculated the proportion of the respective types of disability and the main health, social and economic conditions in two groups, i.e., RTD and other causes of disability (OCD). Differences were adjusted for sex, age group and educational level using logistic regression, with statistical significance being set at p<0.05. The complex sampling design was considered during analysis, which accounts for weighting, clustering, and stratification, by using the “Survey Data” module of the Stata v.12.0 for Windows computer software programme (StataCorp. 2011. Stata Statistical Software: Release 12. College Station, TX: StataCorp LP). Standard errors were computed by using the linearized variance estimator based on a first-order Taylor series. First-order interactions were evaluated between sex and others sociodemographic variables.
ResultsIn 2008, the prevalence of RTD in Spain was 2.1 per 1000 inhabitants; injuries were the fourth cause of disability and within these, traffic accidents ranked second.
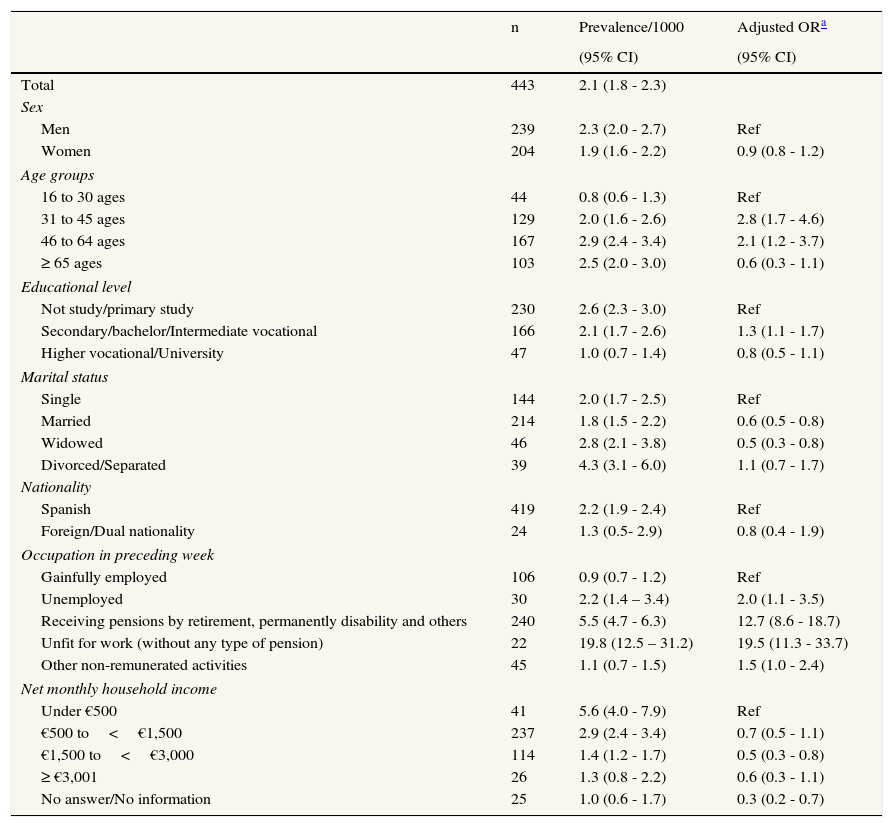
Table 1 shows the distribution of RTD by socio-demographic variables. In comparison with persons aged 16 to 30 years, the odds ratio (OR) of having RTD was higher in the 31-64 year age group and particularly among those aged 31 to 45 years, with an OR of 2.8 (95% CI: 1.7-4.6). There were no statistically significant differences by sex or nationality. Subjects with a secondary education had a higher OR than did those with a primary education or lower (OR=1.3; 95% CI: 1.1-1.7); and married (OR=0.6; 95% CI: 0.5-0.8) and widowed persons (OR=0.5; 95% CI: 0.3-0.8) had a significantly lower OR than did singletons. Nevertheless, there was an interaction between sex and marital status statistically significant: the comparison of married men versus single showed an OR of 0.4 (CI: 0.2-0.5) while women had an OR of 1.7 (1.4-2.8). A breakdown by occupation showed that persons with RTD were more likely to be “unfit for work, without any type of allowance” (OR= 19.5; 95% CI: 11.3-33.7) or “receiving different types of pensions” (OR= 12.7; 95% CI: 8.6-18.7); only 24% were gainfully employed. Persons with household incomes of €1,500 to < €3,000 per month had an OR=0.5 (95% CI: 0.3-0.8) as compared to those with monthly family incomes below €500. Apart from sex and marital status we did not find other statistically significant interactions between sex and sociodemographic variables.
Disability by road traffic crashes according to socio-demographic variables among individuals aged 16 and over. Spain, 2008.
| n | Prevalence/1000 | Adjusted ORa | |
|---|---|---|---|
| (95% CI) | (95% CI) | ||
| Total | 443 | 2.1 (1.8 - 2.3) | |
| Sex | |||
| Men | 239 | 2.3 (2.0 - 2.7) | Ref |
| Women | 204 | 1.9 (1.6 - 2.2) | 0.9 (0.8 - 1.2) |
| Age groups | |||
| 16 to 30 ages | 44 | 0.8 (0.6 - 1.3) | Ref |
| 31 to 45 ages | 129 | 2.0 (1.6 - 2.6) | 2.8 (1.7 - 4.6) |
| 46 to 64 ages | 167 | 2.9 (2.4 - 3.4) | 2.1 (1.2 - 3.7) |
| ≥ 65 ages | 103 | 2.5 (2.0 - 3.0) | 0.6 (0.3 - 1.1) |
| Educational level | |||
| Not study/primary study | 230 | 2.6 (2.3 - 3.0) | Ref |
| Secondary/bachelor/Intermediate vocational | 166 | 2.1 (1.7 - 2.6) | 1.3 (1.1 - 1.7) |
| Higher vocational/University | 47 | 1.0 (0.7 - 1.4) | 0.8 (0.5 - 1.1) |
| Marital status | |||
| Single | 144 | 2.0 (1.7 - 2.5) | Ref |
| Married | 214 | 1.8 (1.5 - 2.2) | 0.6 (0.5 - 0.8) |
| Widowed | 46 | 2.8 (2.1 - 3.8) | 0.5 (0.3 - 0.8) |
| Divorced/Separated | 39 | 4.3 (3.1 - 6.0) | 1.1 (0.7 - 1.7) |
| Nationality | |||
| Spanish | 419 | 2.2 (1.9 - 2.4) | Ref |
| Foreign/Dual nationality | 24 | 1.3 (0.5- 2.9) | 0.8 (0.4 - 1.9) |
| Occupation in preceding week | |||
| Gainfully employed | 106 | 0.9 (0.7 - 1.2) | Ref |
| Unemployed | 30 | 2.2 (1.4 – 3.4) | 2.0 (1.1 - 3.5) |
| Receiving pensions by retirement, permanently disability and others | 240 | 5.5 (4.7 - 6.3) | 12.7 (8.6 - 18.7) |
| Unfit for work (without any type of pension) | 22 | 19.8 (12.5 – 31.2) | 19.5 (11.3 - 33.7) |
| Other non-remunerated activities | 45 | 1.1 (0.7 - 1.5) | 1.5 (1.0 - 2.4) |
| Net monthly household income | |||
| Under €500 | 41 | 5.6 (4.0 - 7.9) | Ref |
| €500 to<€1,500 | 237 | 2.9 (2.4 - 3.4) | 0.7 (0.5 - 1.1) |
| €1,500 to<€3,000 | 114 | 1.4 (1.2 - 1.7) | 0.5 (0.3 - 0.8) |
| ≥ €3,001 | 26 | 1.3 (0.8 - 2.2) | 0.6 (0.3 - 1.1) |
| No answer/No information | 25 | 1.0 (0.6 - 1.7) | 0.3 (0.2 - 0.7) |
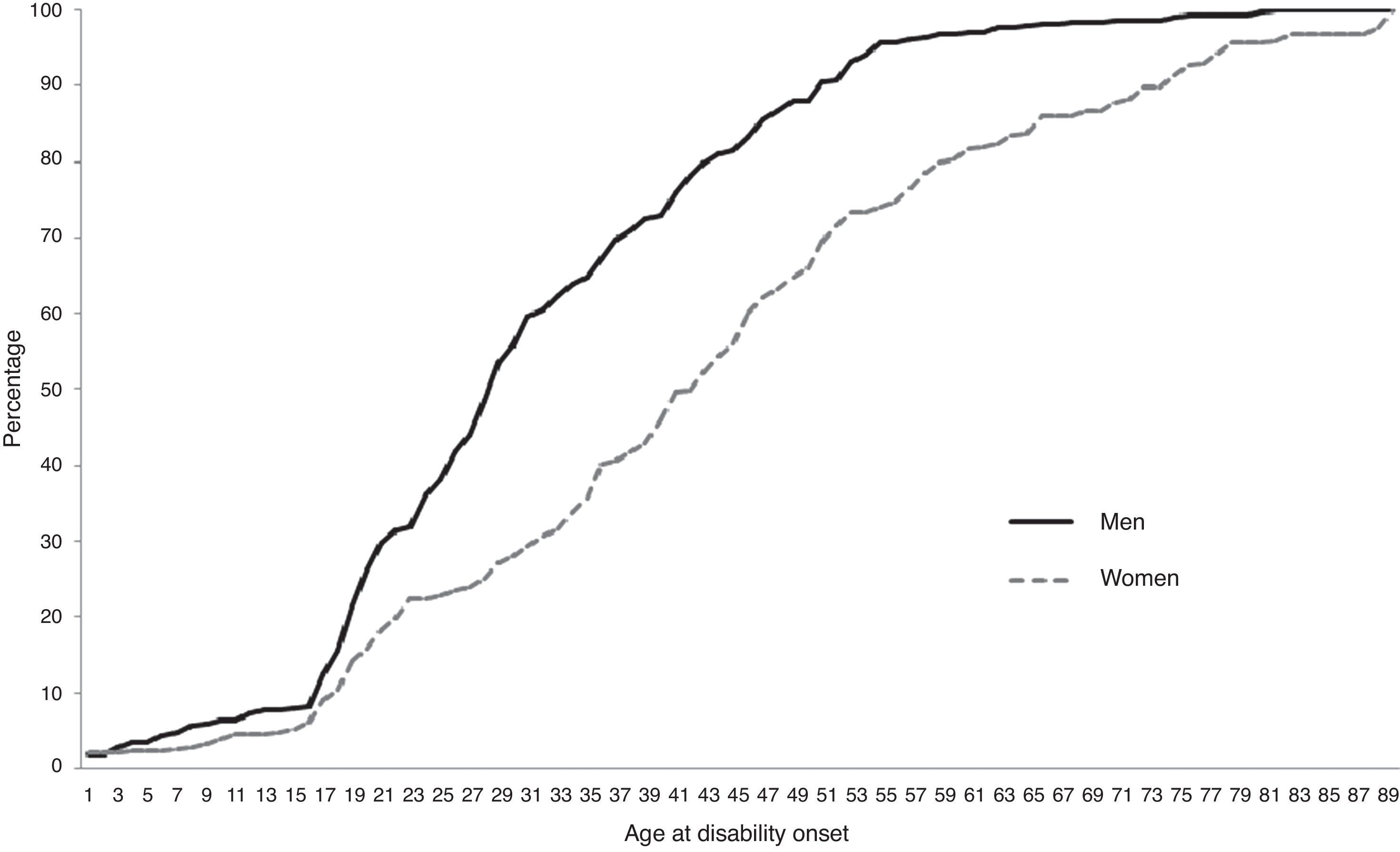
Figure 1 depicts age at disability onset. Seven out of ten persons affected by RTD reported onset of disability before the age of 45 years. The disability onset curve showed an inflection point at age 16 years in both sexes, with onset of disability occurring before the age of 28 years in half of all men and before the age of 40 years in women. This difference of approximately 10 years in RTD onset between men and women remained in evidence up to age 65 years.

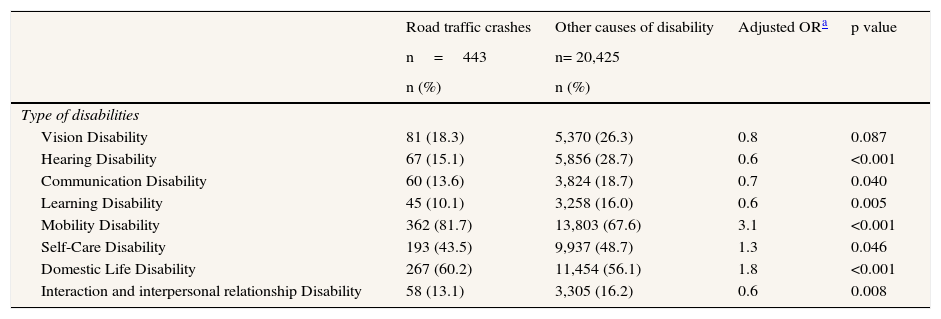
Table 2 describes the type of disability. Mobility, domestic life and self-care were the most frequent types of disability in all disabled persons, and were significantly higher in the case of RTD regarding to other causes of disability (mobility OR=3.1; p<0.001; domestic life OR=1.8; p<0.001; self-care OR=1.3; p=0.046). Hearing (p<0.001), communication (p<0.040), learning (p<0.005) and interaction/interpersonal relationship (p<0.008) disability, were meaningfully lower in the RTD-persons.
Types of Disabilities caused by road traffic crashes and other causes among individuals aged 16 and over. Spain, 2008..
| Road traffic crashes | Other causes of disability | Adjusted ORa | p value | |
|---|---|---|---|---|
| n=443 | n= 20,425 | |||
| n (%) | n (%) | |||
| Type of disabilities | ||||
| Vision Disability | 81 (18.3) | 5,370 (26.3) | 0.8 | 0.087 |
| Hearing Disability | 67 (15.1) | 5,856 (28.7) | 0.6 | <0.001 |
| Communication Disability | 60 (13.6) | 3,824 (18.7) | 0.7 | 0.040 |
| Learning Disability | 45 (10.1) | 3,258 (16.0) | 0.6 | 0.005 |
| Mobility Disability | 362 (81.7) | 13,803 (67.6) | 3.1 | <0.001 |
| Self-Care Disability | 193 (43.5) | 9,937 (48.7) | 1.3 | 0.046 |
| Domestic Life Disability | 267 (60.2) | 11,454 (56.1) | 1.8 | <0.001 |
| Interaction and interpersonal relationship Disability | 58 (13.1) | 3,305 (16.2) | 0.6 | 0.008 |
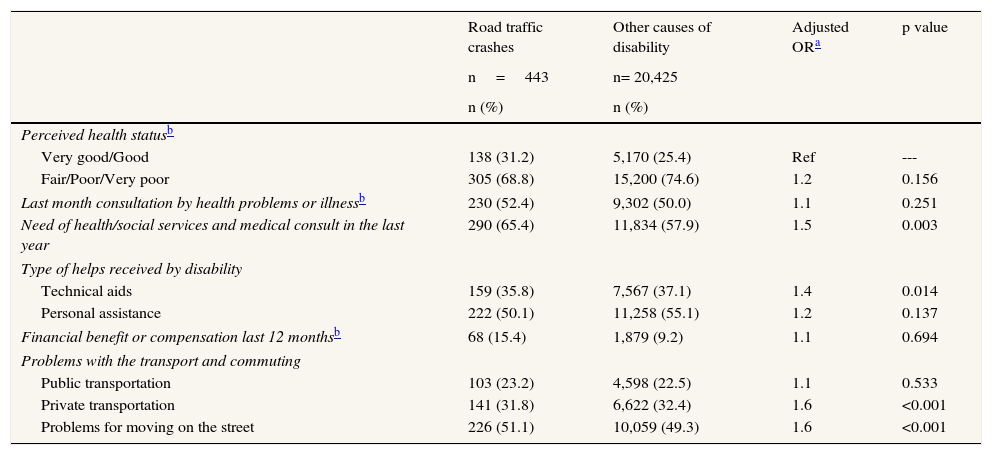
Table 3 shows health and social conditions with respect to disability. Although 68.8% of RTD-sufferers perceived their health status as fair or poor, this percentage was not significant in comparison with the OCD category. Subjects with RTD had a greater need of health/social services (OR=1.5; p=0.003), required more technical aids (OR=1.4; p=0.014), and experienced more problems with private transportation (OR=1.6; p<0.001) and moving around outside the home (OR=1.6; p<0.001).
Health and social conditions of disability caused by road traffic crashes and others causes among individuals aged 16 and over. Spain, 2008..
| Road traffic crashes | Other causes of disability | Adjusted ORa | p value | |
|---|---|---|---|---|
| n=443 | n= 20,425 | |||
| n (%) | n (%) | |||
| Perceived health statusb | ||||
| Very good/Good | 138 (31.2) | 5,170 (25.4) | Ref | --- |
| Fair/Poor/Very poor | 305 (68.8) | 15,200 (74.6) | 1.2 | 0.156 |
| Last month consultation by health problems or illnessb | 230 (52.4) | 9,302 (50.0) | 1.1 | 0.251 |
| Need of health/social services and medical consult in the last year | 290 (65.4) | 11,834 (57.9) | 1.5 | 0.003 |
| Type of helps received by disability | ||||
| Technical aids | 159 (35.8) | 7,567 (37.1) | 1.4 | 0.014 |
| Personal assistance | 222 (50.1) | 11,258 (55.1) | 1.2 | 0.137 |
| Financial benefit or compensation last 12 monthsb | 68 (15.4) | 1,879 (9.2) | 1.1 | 0.694 |
| Problems with the transport and commuting | ||||
| Public transportation | 103 (23.2) | 4,598 (22.5) | 1.1 | 0.533 |
| Private transportation | 141 (31.8) | 6,622 (32.4) | 1.6 | <0.001 |
| Problems for moving on the street | 226 (51.1) | 10,059 (49.3) | 1.6 | <0.001 |
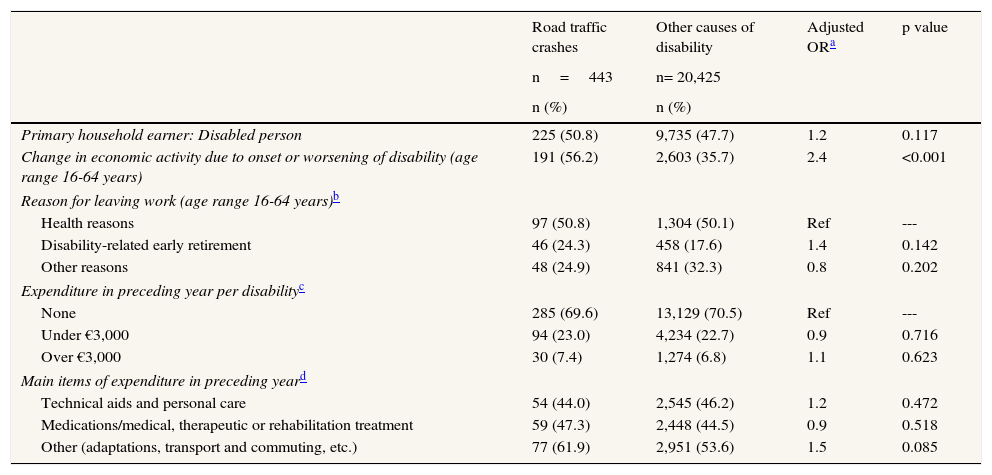
In terms of economic conditions (Table 4), close on 50% of all disabled persons were the primary household earners, with no difference between the RTD and OCD categories. RTD caused major changes in economic activity due to the onset or worsening of disability among persons who were gainfully employed (OR=2.4; p<0.001). Health reasons were the most frequent cause for leaving work; disability-related early retirement was higher among persons in the RTD than among those in the OCD category, but this difference was not significant. No differences were observed in terms of disability-related expenditure and the main items to which such expenditure was allocated.
Economic conditions of disability caused by road traffic crashes and others causes among individuals 16 years and older, Spain 2008.
| Road traffic crashes | Other causes of disability | Adjusted ORa | p value | |
|---|---|---|---|---|
| n=443 | n= 20,425 | |||
| n (%) | n (%) | |||
| Primary household earner: Disabled person | 225 (50.8) | 9,735 (47.7) | 1.2 | 0.117 |
| Change in economic activity due to onset or worsening of disability (age range 16-64 years) | 191 (56.2) | 2,603 (35.7) | 2.4 | <0.001 |
| Reason for leaving work (age range 16-64 years)b | ||||
| Health reasons | 97 (50.8) | 1,304 (50.1) | Ref | --- |
| Disability-related early retirement | 46 (24.3) | 458 (17.6) | 1.4 | 0.142 |
| Other reasons | 48 (24.9) | 841 (32.3) | 0.8 | 0.202 |
| Expenditure in preceding year per disabilityc | ||||
| None | 285 (69.6) | 13,129 (70.5) | Ref | --- |
| Under €3,000 | 94 (23.0) | 4,234 (22.7) | 0.9 | 0.716 |
| Over €3,000 | 30 (7.4) | 1,274 (6.8) | 1.1 | 0.623 |
| Main items of expenditure in preceding yeard | ||||
| Technical aids and personal care | 54 (44.0) | 2,545 (46.2) | 1.2 | 0.472 |
| Medications/medical, therapeutic or rehabilitation treatment | 59 (47.3) | 2,448 (44.5) | 0.9 | 0.518 |
| Other (adaptations, transport and commuting, etc.) | 77 (61.9) | 2,951 (53.6) | 1.5 | 0.085 |
In Spain, RTCs generate two disabled persons per 1,000 population over the age of 15 years. This prevalence rate is lower when compared to data published by other developed countries 10,14–16 but higher in relation to recent Chinese studies,17,18 despite the fact that such information displays important differences in methods, data-sources and type of population analysed. This lower prevalence could be related to the decrease in RTCs with victims, and the ensuing decrease in serious injuries (-43%) in the period 1998-2007.7,9
Although statistics and previously published studies agree on the fact that the greatest number of road accident-related deaths, injuries and disabilities affect young/middle-aged men,1,3,5,9,17–19the profile of the RTD-sufferer in Spain coincides only in terms of age because our study failed to found any significant differences by sex.
As compared to the general population, RTD-sufferers in Spain have a low socio-economic status (worse educational level; lower proportion engaged in gainful employment; high percentage receiving permanent disability retirement or other pensions, unfit for work, and living in the lowest-income households).6 This situation makes them a vulnerable population, with important disadvantages in social aspects: indeed, the socio-economic inequalities in traffic injuries and fatalities have been reported by previous studies,4,17,18,20–23 where the risk of road traffic injuries and fatalities has been shown to be higher among disadvantaged groups with less education,24,25 unskilled occupations,26 lower income27,28 or lower socio-economic status in general.23,28 RTD might thus be aggravating socio-economic disadvantages already present in the population affected, owing -among other things- to important changes in economic activity due to the onset or worsening of disability, health reasons and disability-related early retirement.
Traffic crashes cause 14% more mobility-related disability than do other causes. This could be explained by the type of injury suffered, in that this mainly gives rise to osteoarticular impairments affecting the lower limbs and spinal cord, in line with previous results which show that the musculoskeletal support system, essentially the legs and pelvis, is the region most affected by RTCs.29–31 Assuming that RTCs can generate major injuries and limitations almost immediately, age at disability onset was presumed to be close to the date of the accident, so that our results would suggest that over half of all disabled persons had their accident before the age of 35 years; this figure reinforces and matches previous data, which define the most vulnerable population group as being young adults.1,3,5,9,19,32. However, this information should be interpreted in the context of the age distribution of the sample, where around one in two people have less than fifty years old.
Persons with disability have a considerably more negative self-reported health status than that of the general population6, and this situation holds true for disability caused by RTCs. This condition, taken together with their low socio-economic status, reinforces the idea that socio-economic circumstances, more than other known risk factors, create major differences in health status.33
As Pereda et al. point out, “disabled persons have more need of medical consultation and health/social services than does the general population because they are a group with greater health problems.“6 RTD generates a major need for these types of services/consultation in a group with few technical aids and personal care, which could indicate their degree of involvement and dependence. The RTD-sufferer receives more financial benefits or compensation which could be due to the role of compulsory third-party insurance and indemnity payable to traffic accident victims under the Spanish Motor Vehicle Civil Liability Insurance Act.34 The accessibility and commuting problems of the disabled in Spain have been previously described, with these being shown to be more frequent in the older population (age >65 years).6 RTD-sufferers have a greater risk of experiencing these, a situation that may exacerbate their high degree of mobility-related disability, thereby increasing their level of dependence and limiting their activities in and outside the home.
Although there were no important differences in the expenditure generated by disability, the items of expenditure relating to adaptations, transport, commuting, schooling and housing were the most important in RTD. It would thus seem vital to analyse the social cost of disability caused by RTCs.
Previous studies have ascertained that there is an increased risk of disability following an RTC,16,35 and our results could be suggesting that this risk is especially important in a younger segment of the population. This study was undertaken using a different data source, in order to provide a new view of the problem, complement the information currently available and support the relevance of RTD as a public health problem. Notwithstanding this, there continues to be little scientific information on the subject, and the research that has been conducted indicates a lack of homogeneity in the data sources and the methods applied, which hinders comparisons at an international level.
This study has several limitations and strengths. Among its limitations, the EDAD2008 is a specific survey of disability, which unfortunately does not explore the causes of disability in detail and so does not allow for the characteristics of road traffic crashes to be known. Using the currently available format, information cannot be linked with other RTC databases in order to supplement our existing data. Although the analyses were performed using a complex sample design, it is nevertheless possible that some of the multiple comparisons may have proved significant by chance. Among the study's strengths is the large size and representativeness of the adult population of the country as a whole.
To conclude, prevalence of RTD in Spain is lower than in other developed countries, with middle-aged and socio-economically underprivileged population being at greatest risk. The disadvantages observed in basic socio-economic characteristics, health/social conditions and economic activity make such persons a particularly vulnerable group, with high needs in terms of social and health-care support.
The morbidity and disease burden caused by road traffic crashes (RTCs) are both well documented but their impact on disability has been little studied. There are few studies that use specific disability surveys to describe the consequences of RTCs in terms of disability, and most of these have been conducted in developing countries.
What this study addsThis is the first study on road traffic disability in a southern European country to use population-based disability-specific data and be conducted under the International Classification of Functioning, Disability and Health. It complements information on RTCs and facilitates international comparisons.
Miguel Angel Negrín
Authorship ContributionsR Palmera-Suárez, T López-Cuadrado, R Fernández-Cuenca and I Galán have contributed to the concept and design of the project. J Almazán-Isla and E Alcalde-Cabero have contributed to the collection, review, standardization and appropriateness of databases. R Palmera-Suárez, T López-Cuadrado and I Galán collaborated on the analyses, interpreting the results and writing the article. R Palmera-Suárez, T López-Cuadrado and I Galán had access to all data and are responsible for the overall content. All authors reviewed and approved the final version.
FundingThis study was supported by a grant from the Mutua Madrileña Foundation.
Competing interestNone declared
We are grateful to Diana Gómez-Barroso and Alicia Llácer by their unconditional help and administrative and technical support.











